fetching data ... 
Background: ANCA-associated vasculitides with at least one major item with organ-threatening or life-threatening manifestations are treated according to guidelines for remission induction with rituximab or cyclophosphamide, followed by maintenance therapy, preferably with rituximab [1]. The initial glucocorticoid therapy can be rapidly reduced in dose and significantly shortened by the use of avacopan, a C5 inhibitor, for a treatment duration of approximately 12 months. Under maintenance therapy (usually with RTX), some AAV patients remain in GC-free remission even after discontinuation of avacopan, but there are no long-term observations for this group yet.
Objectives: Prospective observational study on the frequency of relapse in AAV patients undergoing maintenance therapy after discontinuation of GC and AVAC, stratified according to renal and non-renal manifestations.
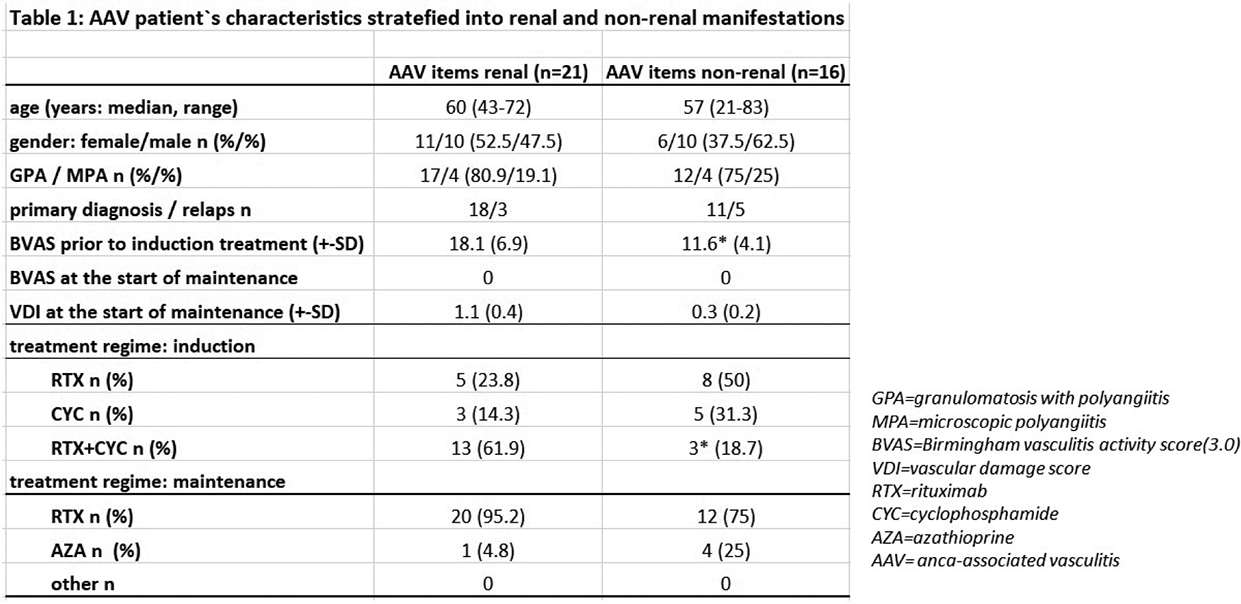
Methods: At the JWK Minden University Hospital, we included 37 AAV patients (n=29 with granulomatosis with polyangiitis, GPA, and 8 with microscopic polyangiitis, MPA) on GC-free maintenance therapy in the prospective study for the observation period between March 2022 and December 2025 to investigate the relapse rate after stopping avacopan. The investigated cohort have been stratefied into AAV patients with versus without renal manifestations. Remission induction was achieved with RTX, CYC, or RTX in combination with CYC, as well as with GC, which was discontinued within 4 months at the latest under avacopan; avacopan itself was discontinued after 9-14 months. The therapy concept was individually adapted by the physician, the follow-up was carried out prospectively every 3 months with determination of the Birmingham Vasculitis Activity Score=BVAS (3.0), VDI (vasculitis damage score) and documentation of any relaps for AAV. Tab.1 shows the characteristics of the AAV patients (n=37) stratified into renal and non-renal manifestations at the time of discontinuation of avacopan. All patients were either PR3 or MPO positive and fulfilled the classification criteria of AAV by ACR/EULAR 2022.
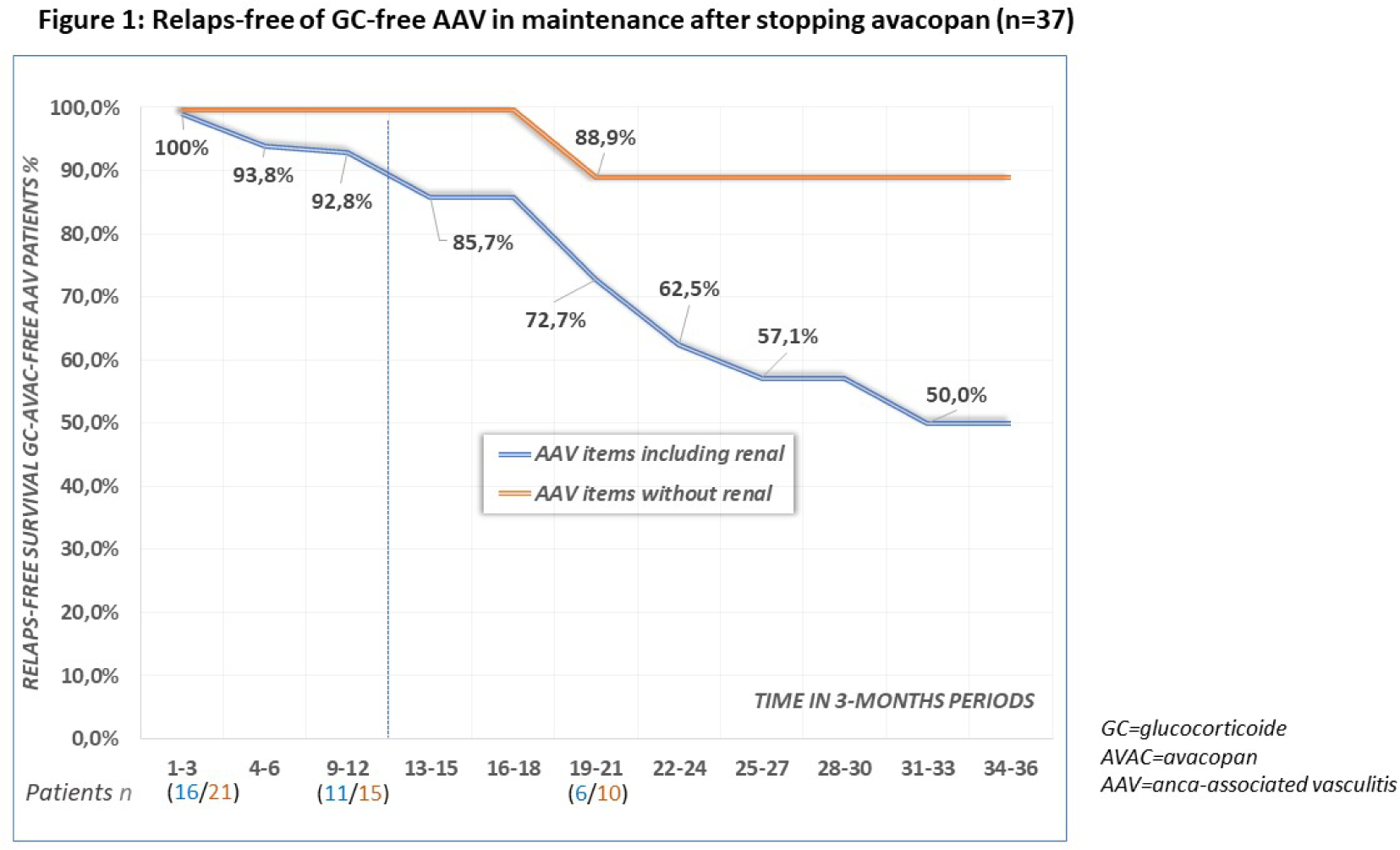
Results: Of the 37 AAV patients, 5 suffered a relapse (13.4%) during the observation mean time 14.6 months, 4 of whom were from the subgroup with non-renal manifestations, although the BVAS score was significantly higher in the subgroup with renal manifestations (18.1 vs. 11.6, p=0.009, t-test). However, this subgroup received intensive induction therapy with RTX in combination with CYC significantly more often (n=13 of 21 versus n=3 of 16, p=0.04; χ-square test). The relapse rate after 12 months was significantly higher in the subgroup with non-renal manifestations (relapse-free survival 100 vs. 85.7%, p=0.01; χ-square test; figure 1).
Conclusions: The vast majority (86.6%) of AAV patients remains in remission 12 months after discontinuing avacopan while receiving GC-free maintenance therapy with RTX or AZA. In this cohort, AAV with non-renal manifestations appears to develop relapses significantly more frequently than renal manifestations. Given the relatively small number of cases and short observation period, it is not possible to conclusively determine the extent to which differences in the induction therapy used or the baseline BVAS score may be responsible for this observation.
REFERENCES: [1] Hellmich B et al, ARD 2024; doi: 10.1136/ard-2022-223764.
Acknowledgments: NIL.
Disclosure of Interests: Gunter Assmann CSL Vifor, Roche Pharma, CSL Vifor, Roche Pharma, Michael Schmidt: None declared, Boll Alina: None declared, Jonas Reimers CSL Vifor, Roche Pharma, CSL Vifor, Roche Pharma, Kerstin Amann: None declared, Radermacher Joerg Roche Pharma, Roche Pharma.