fetching data ... 
Background: Juvenile Idiopathic Arthritis (JIA) requires highly individualized exercise interventions due to its fluctuating disease course and patient-specific functional impacts [1]. While personalized exercise is crucial, traditional supervised delivery faces scalability and long-term adherence challenges [2]). Artificial Intelligence (AI) offers a transformative approach by automating personalized exercise prescription, potentially enhancing patient engagement, goal attainment, and physical activity levels [3]. However, the comparative effectiveness of AI-driven mobile platforms versus supervised AI-integrated clinical settings remains under-explored.
Objectives: This study aimed to compare the effectiveness of a data-driven, AI-based personalized mobile exercise program and a supervised personalized exercise program on functional capacity, physical fitness, gait, and physical activity in adolescents with JIA.
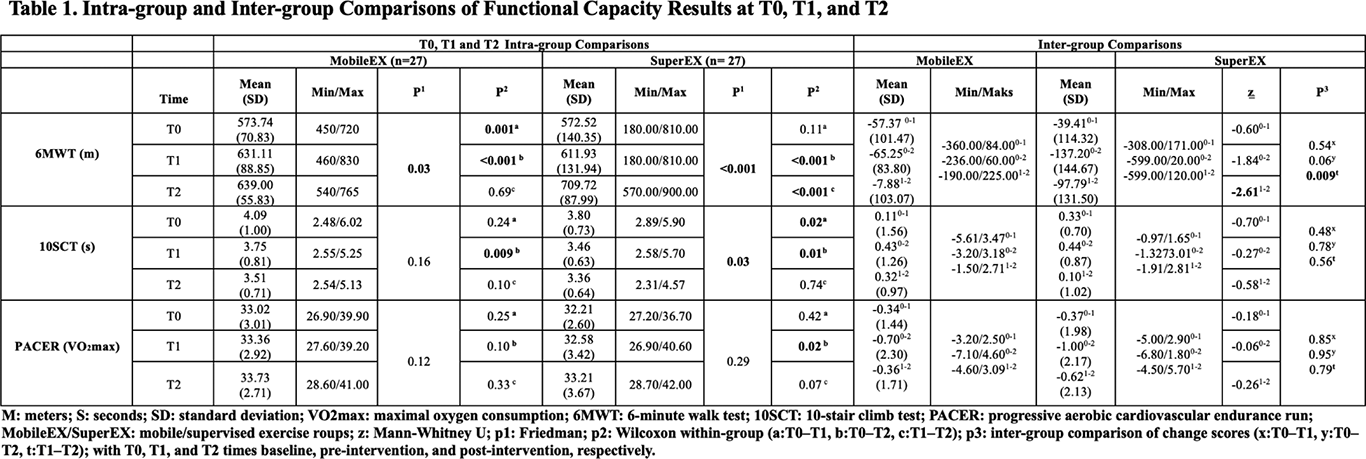
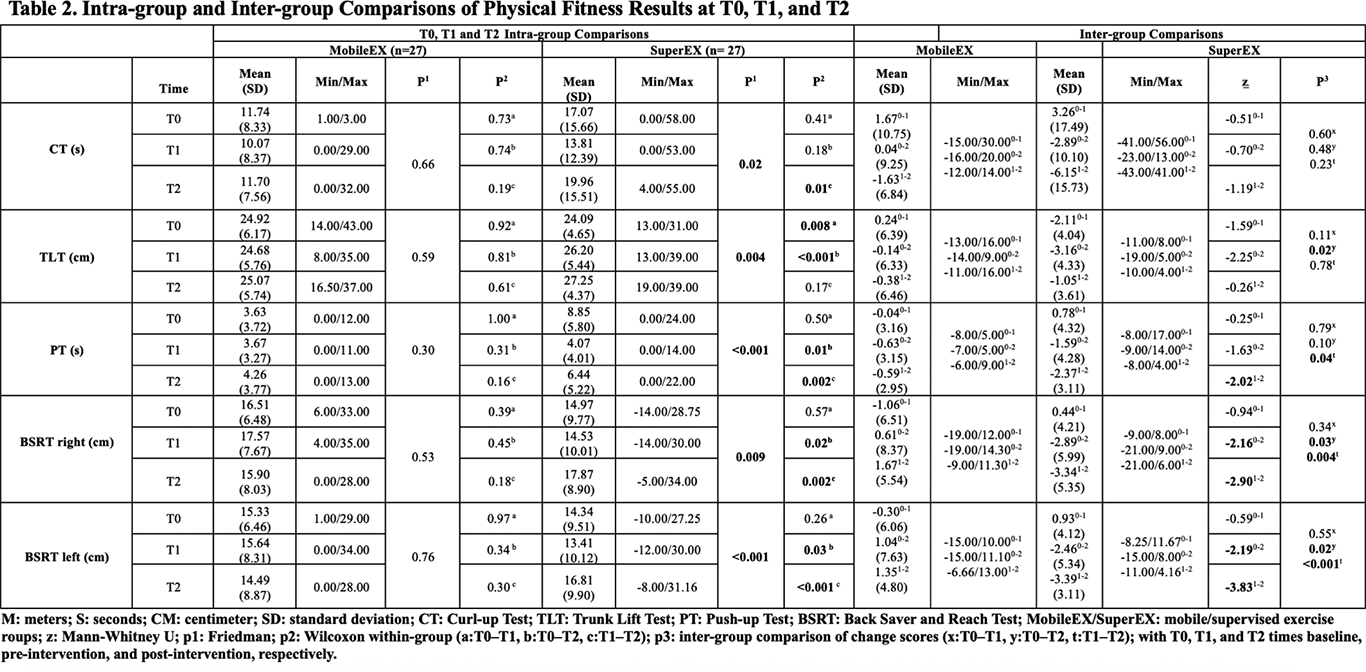
Methods: A total of 54 adolescents with JIA (aged 12-18 years) were randomized into two groups: MobileEX (asynchronous AI-personalized exercise via Pedi@ctivity mobile app) and SuperEX (two supervised clinical and one synchronous online session weekly). The study followed a sequential design: a 3-month baseline monitoring using smartwatches, followed by a 12-week AI-driven exercise intervention (40-45 min/session, 3 times/week). The Pedi@ctivity AI model generated personalized exercise prescriptions for both groups. Outcomes were assessed at baseline (T0), pre (T1), and post-exercise (T2). Functional capacity was measured via 6-Minute Walking Test (6MWT), and 10-Stair Climb Test (10SCT) and Progressive Aerobic Cardiovascular Endurance Run-PACER Test. Physical fitness was assessed using the FitnessGram® Physical Activity Battery (Curl-up-CT, Trunk Lift-TLT, Push-up-PT, Back Saver and Reach-BSRT tests). Gait parameters were evaluated with Digitsole Pro® Smart Insole System. Functional capasity and physical fitness test results were categorized into health zones (Needs Improvement-Health Risk, Needs Improvement, and Healthy Fitness Zone) based on age-matched reference values. Daily physical activity was monitored via smartwatches integrated with the Pedi@ctivity System. Statistical analysis utilized Mann-Whitney U for between-group and Friedman/Wilcoxon tests for temporal comparisons. Clinical significance was evaluated using Cohen’s d for within- and between-group effect sizes (0.20 small, 0.50 medium, >0.80 large) and partial eta squared (η 2 ) for ANOVA interaction effects.
Results: Mean ages were 14.22±1.90 for MobileEX and 15.15±2.08 years for SuperEX. For the 6MWT (T1-T2), SuperEX demonstrated a significantly superior improvement compared with MobileEX (p=0.009, d=0.60), showing a large effect size (d=0.94, η 2 =0.18, p<0.001), whereas MobileEX achieved a moderate-to-large effect (d=0.77, η 2 =0.14, p<0.05). A major clinical breakthrough occurred in ‘Healthy Reference Zone’ transitions for 6MWT, surging from 6 to 19 in SuperEX vs. 7 to 8 in MobileEX. Both groups significantly reduced 10SCT times (MobilEX d=-0.55; SuperEX d=-0.45, p<0.05). Additionally, SuperEX showed significant gains in PACER VO 2max (T0–T2) (d=0.47, η 2 =0.04, p<0.05) (Table 1). In physical fitness T0-T2, SuperEX showed superior gains in trunk extansor strenght/flexibility with TLT (d=0.72, η 2 =0.13, p<0.05), in T1-T2 upper extremity strength with PT (d=0.51, η 2 =0.08, p<0.05) and in T0-T2 and T1-T2, flexibility via BSRT (d=0.95, η 2 =0.21, p<0.05) in (Table 2). Categorical analysis revealed prominent clinical shifts particularly in the SuperEX group. For MT, despite 2 participants regressing, 6 participants in SuperEGZ transitioned from ‘At-Risk’ to the ‘Healthy’ category, reflecting a superior clinical impact compared to the 2-participant improvement in MobileEX. In PT, MobileEX saw 4 participants reach the ‘Healthy’ zone vs. 3 in SuperEX. Furthermore, BSRT categories improved for 2 participants in SuperEX and 1 in MobileEX. Gait kinematics improved significantly in both groups for walking speed (p<0.05), Additionally, the MobileEX also enhanced step length and swing phase duration (p<0.05). For walking speed, SuperEX demonstrated a large effect size (d=0.71, η 2 =0.21), while MobileEX showed a small-to-medium effect (d=0.43, η 2 =0.09). Crucially, no significant between-group differences were found in gait parameters (p>0.05). Smartwatch data showed daily step counts increased significantly only in the SuperEX group (p<0.01). Regression analysis confirmed a positive weekly trend for SuperEX, whereas MobileEX exhibited a negative trajectory. These results suggest that supervised AI-integration effectively sustains long-term activity gains, while the mobile-only approach fails to maintain early progress.
Conclusions: Both programs significantly improved functional capacity, physical fitness, and gait in patiants with JIA. SuperEX demonstrated superior gains in functional outcomes and physical activity, while MobileEX proved a non-inferior, scalable alternative for gait and mobility. These results support a flexible care model: supervised exercise remains optimal when feasible, while mobile platforms provide an effective solution to ensure continuity when clinic access is limited. As the first study to compare these AI-delivery methods in JIA, the findings suggest that AI-integrated physiotherapy enhances both clinical effectiveness and accessibility, potentially bridging long-term care gaps and reducing health inequalities.
REFERENCES: [1] Tarakci, E., et al., 2012, Efficacy of a land-based home exercise programme for patients with juvenile idiopathic arthritis: A randomized, controlled, single-blind study, Journal of Rehabilitation Medicine.
[2] Griffiths, A. J., et al., 2018, The effect of interactive digital interventions on physical activity in people with inflammatory arthritis: A systematic review. Rheumatology International.
[3] Bays, D. K., et al., 2024, A Brief Review of the Efficacy in Artificial Intelligence and Chatbot-Generated Personalized Fitness Regimens, Strength Cond J.
Acknowledgments: NIL.
Disclosure of Interests: None declared.