fetching data ... 
Background: In osteoarthritis (OA), functional impairment is a core disease feature, yet objective and scalable measures of real-world movement remain limited. Most activity-tracker-based studies rely on step counts or daily averages, which summarise overall activity volume but ignore disease-relevant movement patterns such as timing, regularity, and fragmentation. Wearable devices enable continuous, minute-level assessment of physical activity and allow the investigation of daily movement patterns beyond simple averages. Such digital activity-derived measures may provide insight into how people with OA move differently in daily life, even when overall activity levels appear similar.
Objectives: To examine whether activity-derived movement patterns from wearable devices distinguish individuals with OA from those without OA, and to assess whether these patterns reflect functional health and disease severity within the OA population.
Methods: We analysed wrist-worn accelerometer data from adults participating in the US National Health and Nutrition Examination Survey (NHANES 2011–2014; n = 19,931). Adults with self-reported OA were matched 1:1 by age and sex to non-OA participants (1,270 pairs). Participants wore activity monitors continuously for nine days; the first and last day were excluded due to incomplete recording. Minute-level activity data were log-transformed and analysed using harmonic regression to derive movement pattern metrics describing overall activity (mean activity), rhythm strength (24-hour amplitude, A1), day-to-day variability, and timing of peak activity (acrophase, φ1). Linear mixed models assessed group differences and weekday-weekend effects. Circular statistics (Watson-Williams tests) compared acrophase timing. Within the OA group, associations between movement patterns and self-rated general health were analysed.
Results: The matched sample comprised 2,540 participants (mean age 63.0 ± 13.6 years; 64.0% women). Mean overall activity did not differ significantly between OA and non-OA participants (estimate −0.0247, p = 0.097), consistent with previous activity tracker studies. Mean overall activity showed a small, non-significant trend toward lower values in OA (estimate –0.0247, p = 0.097). Across all participants, activity was significantly lower on weekends than weekdays (estimate –0.0850, p < 0.001), with no evidence for a differential weekend effect between OA and non-OA (interaction p = 0.144).
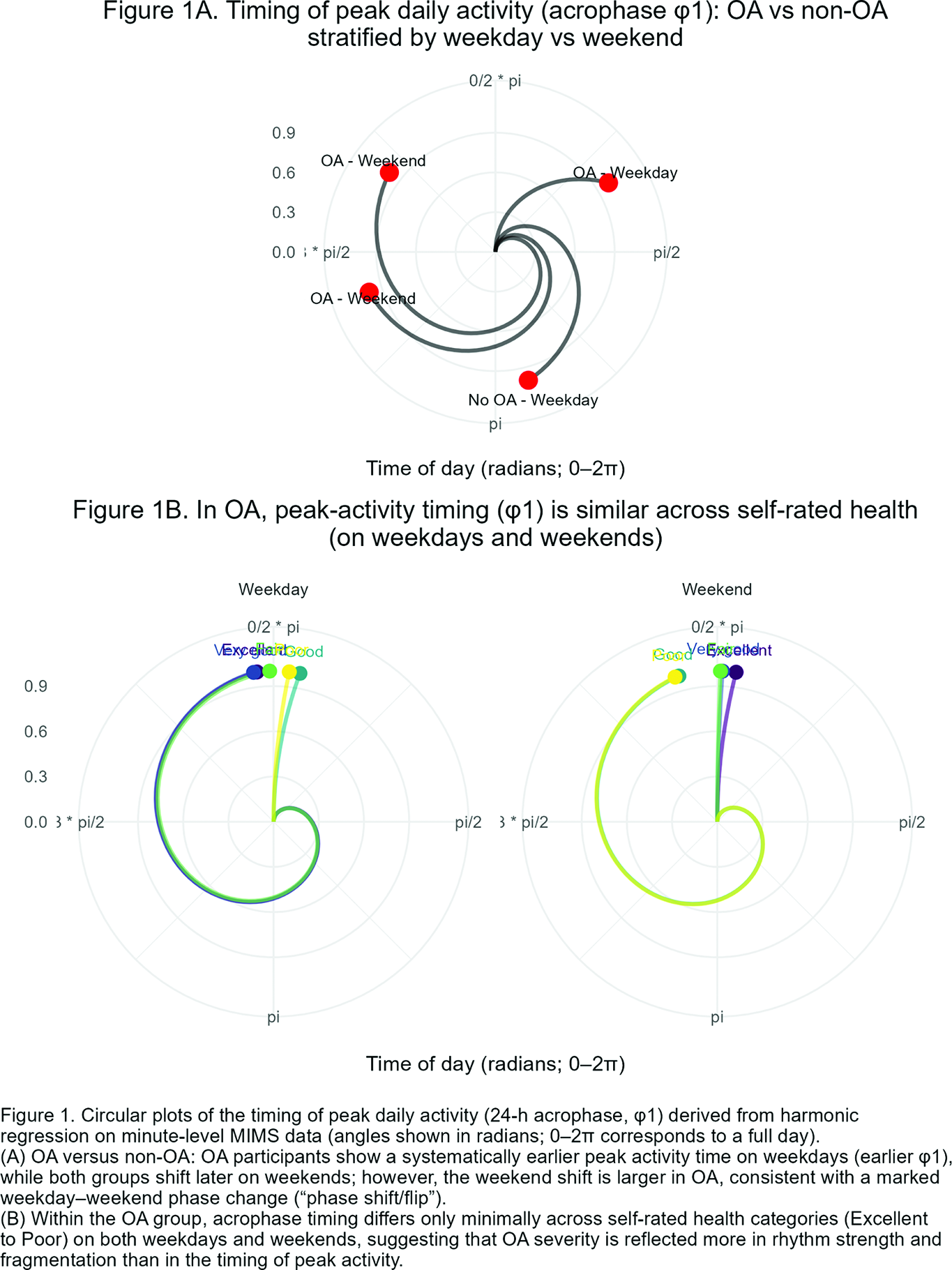
In contrast, pronounced differences emerged in movement timing and daily patterns. On weekdays, participants with OA showed substantially earlier peak activity than non-OA participants (acrophase 1.02 vs. 2.89 radians; F = 1053.5, p < 0.001), corresponding to peak activity around 06:30 versus 11:00. On weekends, both groups shifted toward later activity, but this shift was markedly larger in OA, resulting in a later peak compared with non-OA participants (5.36 vs. 4.40 radians; F = 91.9, p < 0.001). A global four-group comparison (OA × weekday/weekend) confirmed robust differences (F = 2147.7, p < 0.001), indicating a pronounced “phase flip” between weekdays and weekends in OA (Figure 1A).
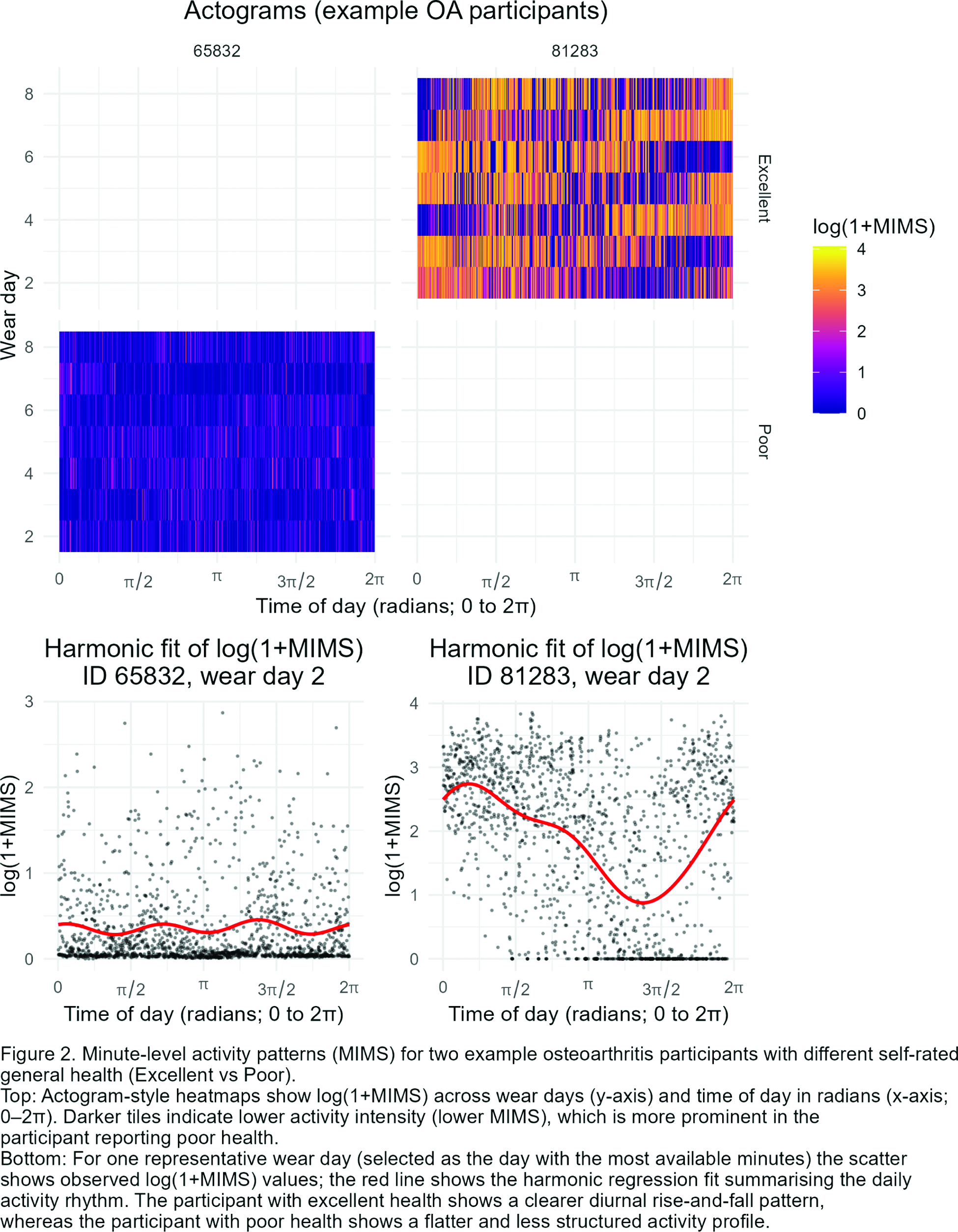
Within the OA group, poorer self-rated general health was associated with lower rhythm strength (24-hour amplitude; β = −0.322, p ≈ 0.003) and higher day-to-day activity variability (β = −0.657, p < 0.001), indicating more fragmented and less regular movement patterns. Overall activity level and timing of peak activity were not independently associated with health status (Figure 1B). Visualisation of minute-level data illustrates distinct daily movement profiles between individuals with excellent versus poor health, despite similar total activity volume (Figure 2).
Conclusions: While average activity levels were similar between OA and non-OA participants, movement patterns differed substantially. Individuals with OA exhibited altered timing and structure of daily activity, including an exaggerated weekday-weekend phase shift. Within OA, poorer health was characterised by weaker and more fragmented movement patterns rather than reduced overall activity. These findings demonstrate that analysing minute-level activity data reveals clinically meaningful differences in movement behaviour that are not captured by step counts or daily averages alone. Activity-derived movement patterns from wearable devices may therefore provide valuable functional markers for OA beyond conventional activity metrics.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Valentin Ritschl: None declared, Valentina Schmolik: None declared, Lisa Dorfer: None declared, Fabian Eibensteiner: None declared, Tanja Stamm Personal fees from Sanofi, Takeda and Novartis, outside the submitted work., Grants and personal fees from AbbVie and Roche, outside the submitted work.