fetching data ... 
Background: Juvenile Idiopathic Arthritis (JIA) is associated with chronic inflammation and pain, which may contribute to kinesiophobia and reduced physical activity [1,2,3]. Sustained inactivity can further compromise muscle strength, physical fitness, and health-related quality of life [3,4].
Objectives: This study compared the effects of a structured core stabilization exercise program and an exergaming-based core stabilization program on pain, fatigue, functional capacity, physical fitness, and muscle strength in children with JIA.
Methods: Thirty children with JIA (8-12 years) were randomized to a structured core stabilization group (Group 1, n=15) and an exergaming-based core stabilization group (Group 2, n=15). Both groups completed a progressive 12-week programme (2 sessions/week; 45–50 min/session; easy–medium–hard progression). Outcomes assessed pre- and post-intervention included pain and fatigue (Numeric Rating Scale), functional capacity (6-minute walk test [6MWT], 30-second sit-to-stand [30STS], 10-step climbing test [10SCT]), physical fitness (Fitnessgram Battery), and muscle strength parameters. Exercise satisfaction and perceptions were explored using structured scoring and open-ended questions.
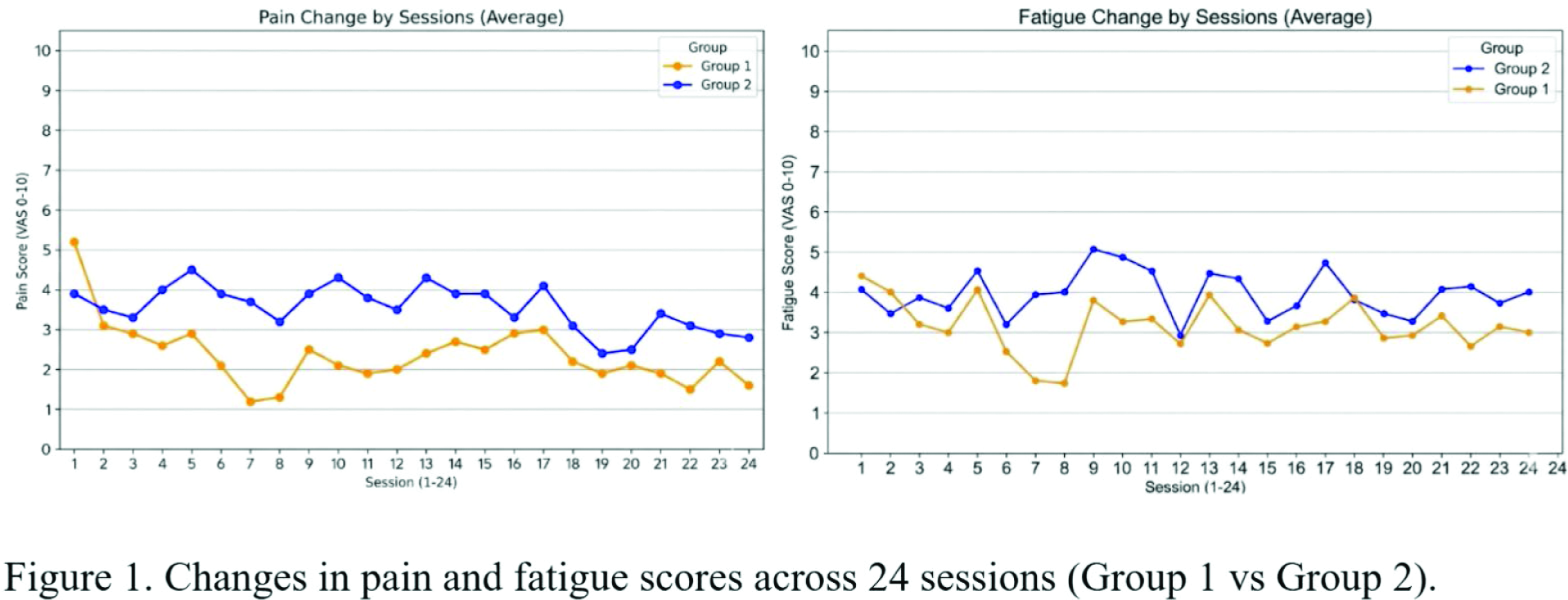
Results: Overall, pain and fatigue scores remained generally stable across both groups despite progressive increases in exercise difficulty; however, level-specific changes were observed. Pain and fatigue changes across 24 sessions were shown in Figure 1. In Group 1, pain decreased significantly at the easy and hard levels, and fatigue decreased significantly at the easy level, whereas fatigue increased significantly during the transition from easy to medium level of exercise program. In Group 2, pain and fatigue scores remained stable across all difficulty levels. Between-group comparisons indicated a significantly greater change in pain and fatigue at the easy level in Group 1. Exercise satisfaction was high in both groups. All functional capacity and physical fitness outcomes were presented in Table 1.
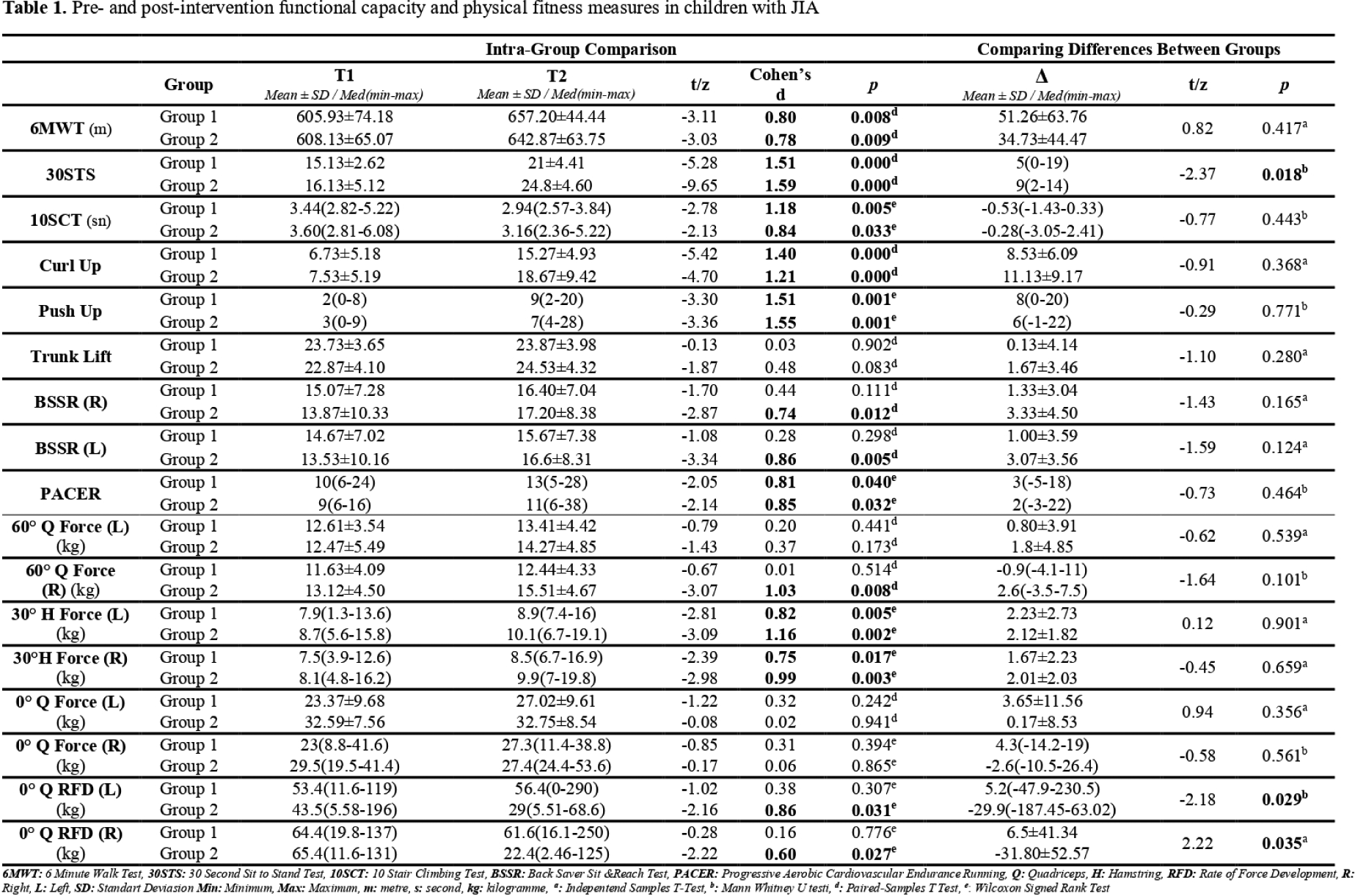
Functional Capacity: Significant within-group improvements were observed in 6MWT, 30STS, and 10SCT in both groups (p<0.05). In between-group comparisons, Group 2 demonstrated superior improvement in 30STS (p<0.05; Cohen’s d=0.96).
Physical Fitness: Significant and comparable improvements were detected in curl-up, push-up, and PACER tests in both groups. A statistically significant increase in flexibility (Back-Saver Sit-and-Reach) was observed only in Group 2 (p<0.05).
Fitnessgram Categories: Based on Fitnessgram reference standards, the number of participants classified within the “Healthy Fitness Zone” increased markedly post-intervention in both groups, particularly for curl-up and push-up tests (majority reaching n=10–13). Positive transitions from the “Needs Improvement/At-risk” categories to the “Healthy Fitness Zone” were also observed for Trunk Lift and Sit-and-Reach parameters.
Muscle Strength: At 30°, hamstring strength increased significantly in both groups (p<0.05). A significant increase in 60° quadriceps strength with a very large effect size was observed only in Group 2 (d=1.03). Peak force at 0° did not change in either group; however, RFD at 0° decreased significantly in Group 2 compared with Group 1 (p<0.05), which may indicate a shift toward more controlled force production rather than explosive contraction.
Group 2 (Qualitative feedback): Feedback most frequently emphasized perceived “pain reduction,” “postural improvement,” and “endurance.” Notably, despite stable quantitative pain scores, children commonly reported subjective symptom relief.
Group 1 (Qualitative feedback): Feedback predominantly highlighted “physical strengthening,” with participants reporting regional improvements (e.g., legs/knees) and increased energy. Although clinical pain scores decreased significantly, “pain reduction” was not a prominent theme in verbal feedback.
Conclusions: In children with JIA, both structured core stabilization and exergaming-based core stabilization programmes were feasible, well accepted, and associated with improvements in functional capacity and physical fitness without worsening overall pain or fatigue despite progressive workload. Compared with structured training, the exergaming programme showed additional benefits in dynamic functional performance (30STS), flexibility, and 60° quadriceps strength, alongside more favorable symptom-related perceptions in qualitative feedback. The observed reduction in RFD in the exergaming group may reflect a shift toward controlled force production, which could be consistent with joint protection–oriented neuromuscular adaptation. Taken together, exergaming may serve as a valuable adjunct to conventional rehabilitation by supporting engagement and potentially addressing psychological barriers such as kinesiophobia.
REFERENCES: [1] Bilginer, Y., 2019, Juvenil İdiyopatik Artrit, Türkiye Çocuk Hastaliklari Dergisi, 13 (4), 221–221.
[2] Woolnough, L. U., Lentini, L., Sharififar, S., Chen, C., ve Vincent, H. K., 2022, The relationships of kinesiophobia and physical function and physical activity level in juvenile idiopathic arthritis, Pediatric Rheumatology, 20 (1).
[3] Fazaa, A., Sellami, M., Ouenniche, K., Miladi, S., Kassab, S., Chekili, S., Ben Abdelghani, K., ve Laatar, A., 2021, Physical activity assessment in children and adolescents with juvenile idiopathic arthritis compared with controls, Archives de Pédiatrie, 28 (1), 47–52.
[4] Woolnough, L., Pomputius, A., ve Vincent, H. K., 2021, Juvenile idiopathic arthritis, gait characteristics and relation to function, Gait & Posture, 85, 38–54.
Acknowledgments: NIL.
Disclosure of Interests: None declared.