fetching data ... 
Background: Psoriatic arthritis (PsA) is a chronic inflammatory disease that significantly impacts joint function and quality of life. Accurate assessment of structural damage is essential for monitoring disease progression and evaluating treatment efficacy in clinical trials [1]. Radiographic scoring using the PsA-modified van der Heijde Sharp (vdHS) [2] method remains the gold standard but is labor-intensive, costly, and requires specialized expertise. While deep learning approaches have shown promise in automating scoring, their capacity to capture longitudinal changes in PsA joint damage remains largely unexplored, primarily due to the difficulty of detecting subtle changes over short clinical trial intervals.
Objectives: To develop and evaluate Sharp.AI, an end-to-end deep learning pipeline that leverages longitudinal radiographic information to improve automated scoring of bone erosion (BE) and joint space narrowing (JSN) in PsA for measuring structural progression over time.
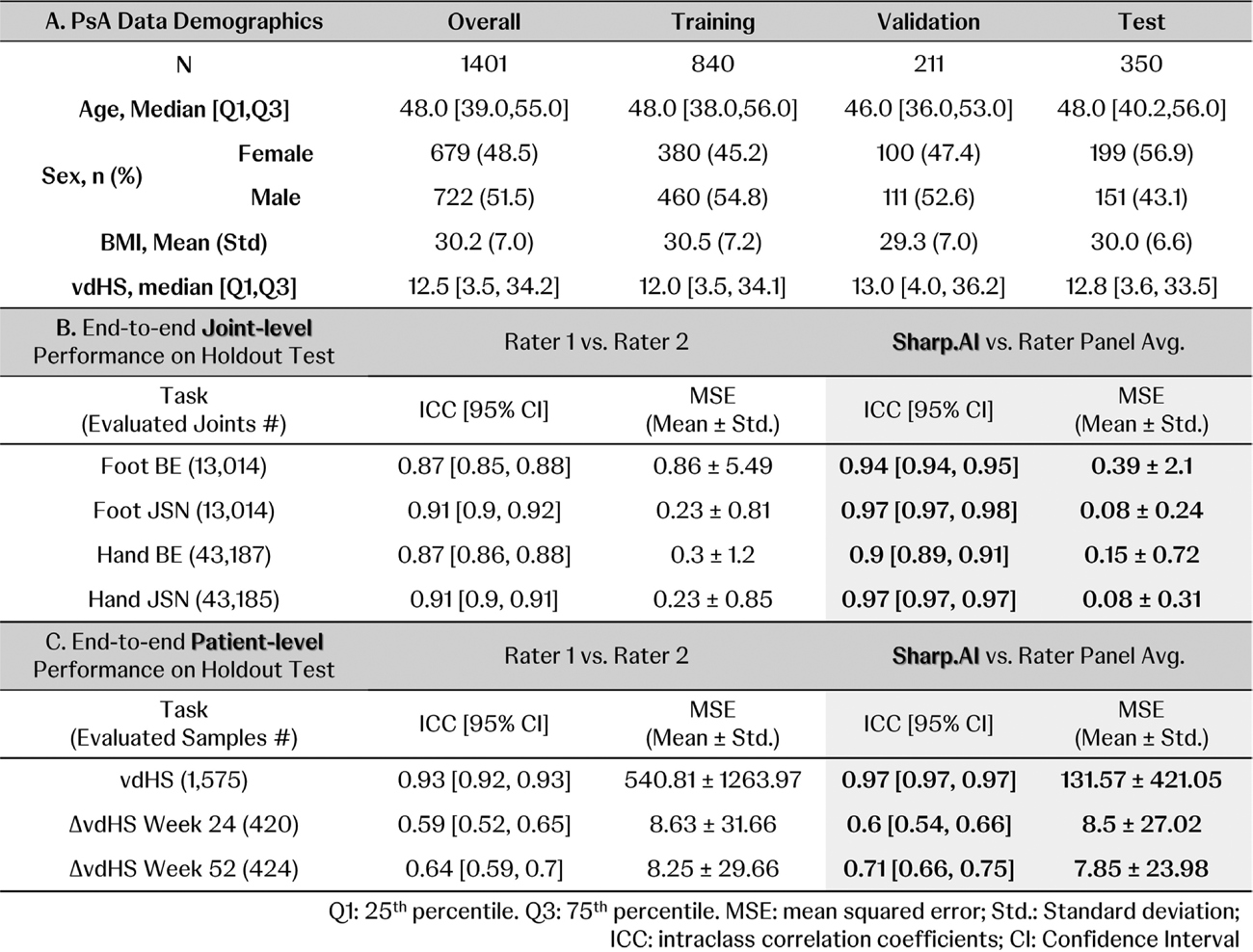
Methods: Radiographs from three PsA clinical trials (1,401 patients; 17,430 X-rays) and three RA trials (2,749 patients; 44,794 X-rays) were used. A patient-wise stratified split allocated 2,153 RA patients (37,242 images) and 1,051 PsA patients (13,055 images) for training and validation, while 350 PsA patients (4,375 images) were reserved as a hold-out test set. Demographics of the PsA dataset are presented in Table 1A. To train, optimize, and evaluate the pipeline, a subset of PsA images (8,546 foot and 1,804 hand X-rays) was annotated with bounding boxes around joints scored in the vdHS method. Additionally, vdHS scores and joint-level sub-scores from clinical trials, provided by two radiologists and an adjudicator, served as ground truth for the scoring models and were available across all PsA images.
The Sharp.AI pipeline (Figure 1A) consisted of three key modules:
Foundation model: Built using 720,762 joint image patches from PsA and RA datasets, enabling the model to learn general joint patterns.
Joint Detection (JD): Applied advanced detection algorithms to automatically identify and localize hand and foot joints in X-rays.
Auto-Scoring (ASC) models: Fine-tuned on foundation model to evaluate bone erosion (BE) and joint space narrowing (JSN) in hands and feet joints. It not only learned to produce joint-level scores for individual visits but also incorporated a strategy to ensure predicted changes aligned with actual changes (Δ) across visits.
The Sharp.AI pipeline was evaluated on the PsA hold-out test set at both joint and patient levels. The locked JD model performed joint localization, while the locked ASC models generated scores. Joint-level scores were accumulated to produce patient-level results, and changes in vdHS scores (ΔvdHS) were calculated based on vdHS differences across visits. Evaluation metrics included intraclass correlation coefficient (ICC) and mean squared error (MSE), using expert panel scores as the reference and comparing results against two individual raters. Model interpretability was examined through attention maps generated by the ASC models.
Results: The Sharp.AI pipeline demonstrated strong performance at the joint level for both BE and JSN tasks (Table 1B). For foot joints, the BE task achieved an ICC of 0.94 against the panel average and an MSE of 0.38 ± 2.10, compared to inter-rater ICC of 0.87 and MSE of 0.86 ± 5.49. For JSN, the model reached an ICC of 0.97 with an MSE of 0.08 ± 0.24, while human raters achieved ICC of 0.91 and MSE of 0.23 ± 0.81. For hand BE task, the model showed ICC of 0.90 and MSE of 0.15 ± 0.72 versus human ICC of 0.87 and MSE of 0.30 ± 1.20. For JSN on hands, the model achieved ICC of 0.97 and MSE of 0.08 ± 0.31, compared to inter-rater ICC of 0.91 and MSE of 0.23 ± 0.85. At the patient level (Figure 1B; Table 1C), Sharp.AI achieved ICC of 0.97 against panel average vdHS scores with MSE of 131.57 ± 421.05, outperforming inter-expert agreement (ICC of 0.93 and MSE of 540.81 ± 1263.97). For ΔvdHS prediction (Figure 1C; Table 1C), the model also surpassed human raters. At Week 24, model versus panel average achieved ICC of 0.60 and MSE of 8.50 ± 27.02, compared to inter-rater ICC of 0.59 and MSE of 8.63 ± 31.66. At Week 52, the model reached ICC of 0.71 and MSE of 7.85 ± 23.98, while human raters achieved ICC of 0.64 and MSE of 8.25 ± 29.66. Attention maps confirmed that the model focused on clinically relevant joint regions (Figure 1D).
Conclusions: Sharp.AI demonstrates state-of-the-art performance in automated PsA radiographic scoring and introduces a novel longitudinal approach that accurately captures score changes over short time intervals at Week 24 and Week 52. This method provides a scalable, objective alternative to manual scoring, with the potential to accelerate clinical trial workflows and improve consistency in monitoring structural joint damage.
Sharp.AI pipeline and performance evaluation. A. Schematic diagram of the Sharp.AI pipeline for patient-level vdHS score prediction. B. Sharp.AI performance at the patient level for vdHS score prediction. Left—Sharp.AI predictions vs. rater panel average; Right—individual rater assessments (Rater 1 vs. Rater 2). C. Sharp.AI performance on vdHS score change. Left: from screening to Week 24; Right: from screening to Week 52. D. Attention maps generated by the ASC model for foot (upper panel) and hand (lower panel) images. Left: original radiograph; Middle: BE attention map highlighting regions associated with bone erosion; Right: JSN attention map showing model focus on joint space and overall joint size for joint space narrowing assessment.
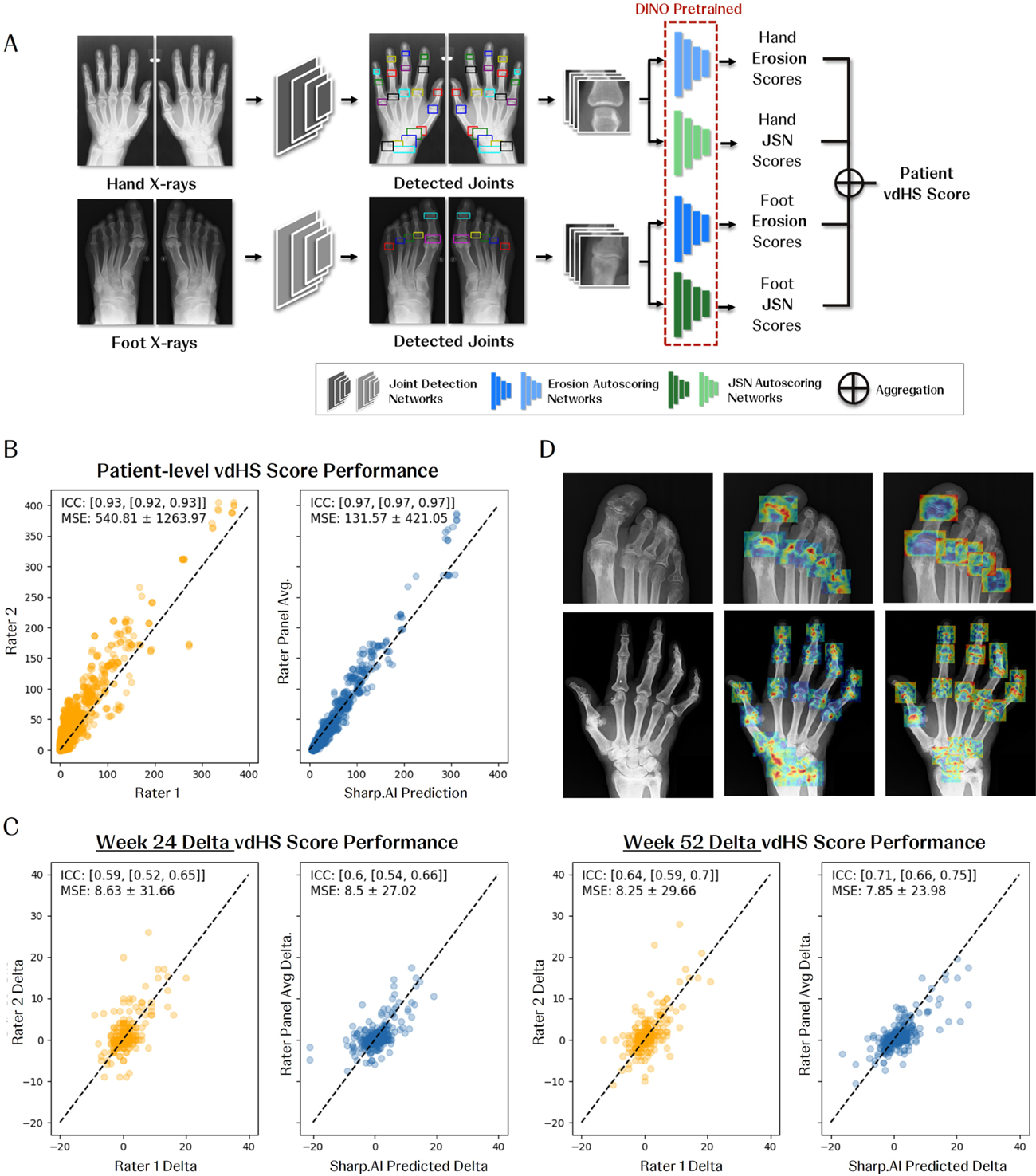
Table 1. Patient Demographic and Quantitative Performance of the Sharp.AI Pipeline.
REFERENCES: [1] Van Der Heijde, D., et al., Assessing structural damage progression in psoriatic arthritis and its role as an outcome in research. Arthritis research & therapy, 2020
[2] Van der Heijde, D., et al., Psoriatic arthritis imaging: a review of scoring methods. Annals of the Rheumatic Diseases, 2005
Acknowledgments: NIL.
Disclosure of Interests: Zijun Gao may own stock or stock options in J&J, employee of J&J, Darshana Govind may own stock or stock options in J&J, employee of J&J, Dimitri Kessler was an employee of J&J, Chaitanya Parmar may own stock or stock options in J&J, employee of J&J, Kenneth Broos may own stock or stock options in J&J, employee of J&J, Nicholas Fountoulakis may own stock or stock options in J&J, employee of J&J, Xiaoqin Tang may own stock or stock options in J&J, employee of J&J, Luiza Gabriel may own stock or stock options in J&J, employee of J&J, Elizabeth C. Hsia may own stock or stock options in J&J, was employee of J&J, Gabriela Oana Cula may own stock or stock options in J&J, employee of J&J, Lenore Noonan may own stock or stock options in J&J, employee of J&J, Philip S. Murphy may own stock or stock options in J&J, employee of J&J, Anna Beutler may own stock or stock options in J&J, employee of J&J, Terence Rooney may own stock or stock options in J&J, employee of J&J, Peter Ory: None declared, Michael Deman may own stock or stock options in J&J, employee of J&J, Kristopher Standish may own stock or stock options in J&J, employee of J&J, Robert Janiczek may own stock or stock options in J&J, employee of J&J.