fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease associated with substantial comorbidity and premature mortality. Marked ethnic disparities exist in disease severity, comorbidity burden, and outcomes; however, most evidence derives from specialist cohorts, limiting generalisability to the wider SLE population. Greater Manchester is one of the most ethnically and socioeconomically diverse regions in the United Kingdom, providing an important setting for population-level lupus research. The Greater Manchester Care Record (GMCR) integrates primary care clinical and prescribing data for approximately 2.8 million residents, offering a unique opportunity to characterise real-world SLE across the full spectrum of disease severity and care settings.
Objectives: To describe a prevalent cohort of patients with SLE in Greater Manchester, with a focus on comorbidities, infections, vaccination uptake, and medication use across ethnic groups.
Methods: We conducted a retrospective analysis of anonymised routinely collected healthcare data from the GMCR. Patients with SLE who were alive on 1 January 2025 were included. Demographic characteristics, comorbidities, hospital attendances for infections, vaccination records, and medication use were extracted from primary care records. Hospital prescribing data were not available. Age-adjusted prevalence estimates were calculated using 2021 UK Census population data.
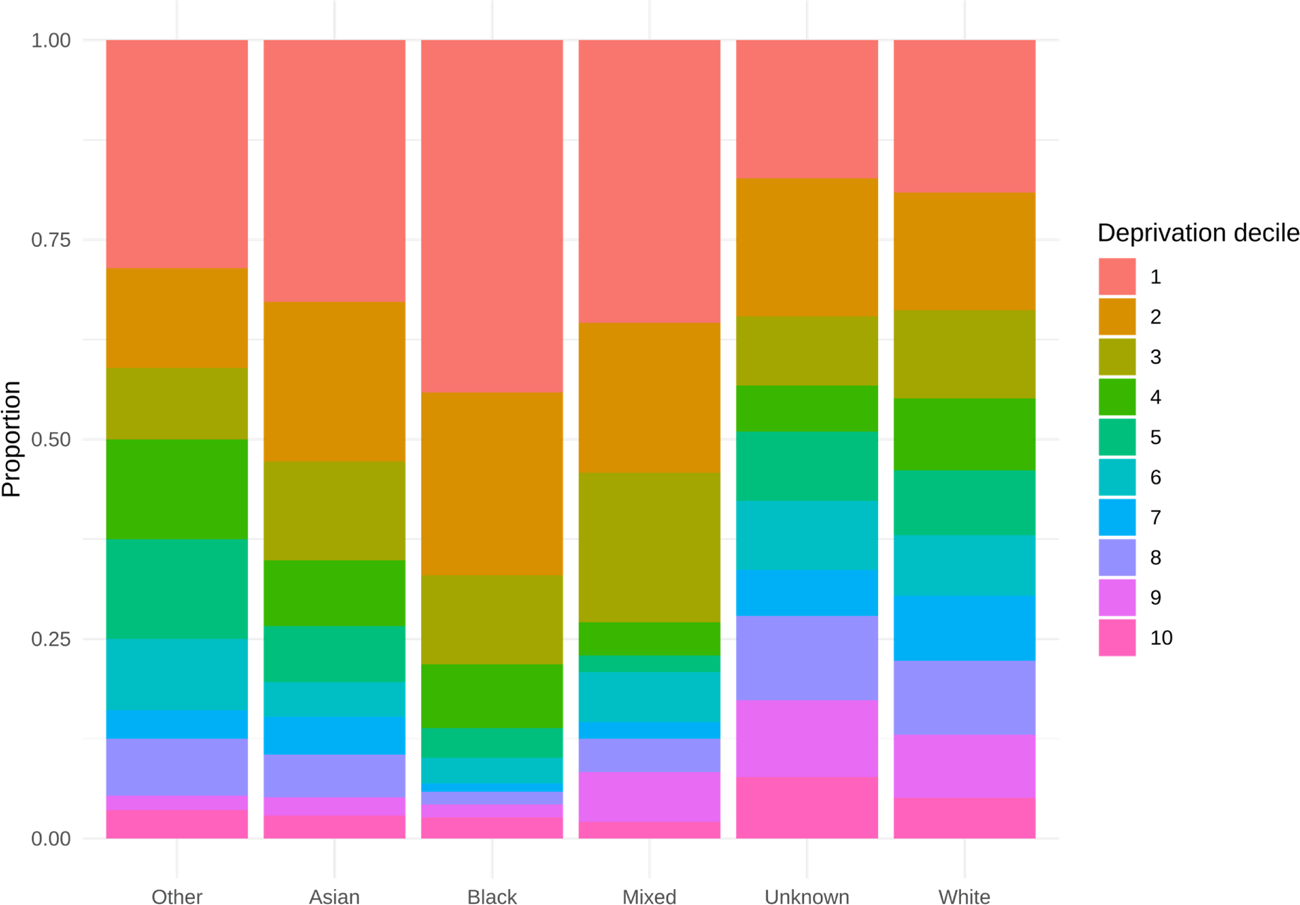
Results: We identified 2,727 SLE patients (2,403 female [88%]; median age 57 years [IQR 43–68]; median disease duration 13.2 years [IQR 6.2–22.8]). Ethnic distribution was White 1,846 (67.7%), Asian 485 (17.8%), Black 188 (6.9%), and Mixed/Other/Unknown 208 (7.6%). Age-adjusted prevalence per 100,000 was highest in Black patients (140.2) and Asian patients (124.6) versus White patients (84.3). Socioeconomic deprivation was greater among Black (126/188 [67%] in lowest quintile), Asian (256/485 [52.8%]), compared to White (624/1846 [33.8%]), Figure 1. Lupus nephritis was most common in Black (38/188 [20.2%]) and Asian (73/485 [15.1%]) patients. Cardiometabolic comorbidities included hypertension (925/2,727 [33.9%]), chronic kidney disease (330/2,727 [12.1%]), type 2 diabetes (318/2,727 [11.7%]), and coronary heart disease (241/2,727 [8.8%]). Mental health comorbidities included anxiety (811/2,727 [29.7%]) and depression (147/2,727 [5.4%]). Infection incidence was 455/1,000 patient-years in primary care (19,110 infections in 2,199 patients) and 79.5/1,000 patient-years in hospital settings (3,338 infections in 947 patients). Vaccination uptake varied by ethnicity: influenza in the preceding year was highest among White patients (1,090/1,846 [59%]) versus Asian (191/485 [39.4%]) and Black patients (70/188 [37.2%]); COVID-19 vaccination in the preceding year was 767/1,846 (41.5%) in White versus 60/485 (12.4%) in Asian and 27/188 (14.4%) in Black patients. Current immunosuppressive therapy was prescribed in 475/2,727 (17.4%), and hydroxychloroquine in 1,046/2,727 (38.4%) in primary care, and use was higher in Black and Asian patients. Oral corticosteroid (OCS) use in the preceding year was 952/2,727 (34.9%), with 428/2,727 (15.7%) receiving >5 mg daily and 321/2,727 (11.8%) >10 mg daily. Frequent OCS use since diagnosis was more common in Black (64/188 [34.0%]) and Asian (160/485 [33.0%]) patients compared with White patients (384/1,846 [20.8%]).
Conclusions: In this population-based, multi-ethnic SLE cohort, comorbidities, infections, and corticosteroid exposure were common. Black and Asian patients experienced earlier disease onset, higher cumulative steroid exposure, greater deprivation, and a higher burden of renal and cardiometabolic comorbidities. These findings demonstrate the value of population-level electronic health records in identifying health inequities in SLE and highlight the need for targeted strategies to improve outcomes beyond specialist care settings.
| Asian or Asian British (N=485) | Black, African, Caribbean or Black British (N=188) | Unknown/ Other (N=208) | White British (N=1846) | Overall (N=2727) | |
|---|---|---|---|---|---|
| Female, N(% ) | 429 (88.5%) | 167 (88.8%) | 192 (92.3%) | 1615 (87.5%) | 2403 (88.1%) |
| Age (years), median (IQR ) | 45.0 [36.0, 57.0] | 49.0 [35.0, 59.0] | 47.0 [35.0, 58.2] | 61.0 [50.0, 72.0] | 57.0 [43.0, 68.0] |
| Age at diagnosis, median (IQR ) | 34.0 [25.0, 43.0] | 35.0 [27.0, 45.0] | 34.0 [24.0, 45.0] | 42.0 [31.0, 52.0] | 39.0 [29.0, 50.0] |
| IMD 2019 most deprived quintile, N(% ) | 256 (52.8%) | 126 (67.0%) | 85 (40.9%) | 624 (33.8%) | 1091 (40.0%) |
| Smoking Status, N(% ) | |||||
| Current | 22 (4.5%) | 11 (5.9%) | 32 (15.4%) | 309 (16.7%) | 374 (13.7%) |
| Ex | 29 (6.0%) | 28 (14.9%) | 35 (16.8%) | 652 (35.3%) | 744 (27.3%) |
| Never | 407 (83.9%) | 143 (76.1%) | 126 (60.6%) | 871 (47.2%) | 1547 (56.7%) |
| BMI, median (IQR ) | 25.6 [22.2, 30.1] | 28.2 [24.8, 33.9] | 26.6 [22.4, 31.6] | 26.7 [23.0, 31.4] | 26.6 [22.8, 31.3] |
| Disease duration, median (IQR ) | 9.5 [3.3, 16.1] | 9.0 [3.6, 15.4] | 9.0 [3.1, 19.1] | 16.4 [8.3, 24.8] | 13.2 [6.2, 22.8] |
| Lupus nephritis, N(% ) | 73 (15.1%) | 38 (20.2%) | 23 (11.1%) | 104 (5.6%) | 238 (8.7%) |
| Chronic kidney disease, N(% ) | 41 (8.5%) | 25 (13.3%) | 20 (9.6%) | 244 (13.2%) | 330 (12.1%) |
| Type 2 diabetes mellitus, N(% ) | 69 (14.2%) | 22 (11.7%) | 19 (9.1%) | 208 (11.3%) | 318 (11.7%) |
| Influenza vaccine (last 12 months), N(% ) | 191 (39.4%) | 70 (37.2%) | 72 (34.6%) | 1090 (59.0%) | 1423 (52.2%) |
| Covid vaccine (last 12 months), N(% ) | 60 (12.4%) | 27 (14.4%) | 46 (22.1%) | 767 (41.5%) | 900 (33.0%) |
| Hospital infections, per 1000 patient years | 96.1 | 133.1 | 125.3 | 70.0 | 79.5 |
| Antimalarial (current ) | 244 (50.3%) | 104 (55.3%) | 75 (36.1%) | 623 (33.7%) | 1046 (38.4%) |
| Immunosuppression (current ) | 124 (25.6%) | 58 (30.9%) | 41 (19.7%) | 252 (13.7%) | 475 (17.4%) |
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Sarah Dyball: None declared, Mia Rodziewicz: None declared, Ian Bruce Astra Zeneca, Janssen, GSK, Novartis, Astra Zeneca, Janssen, GSK, Novartis, Takeda, BMS, Grants to institution from Astra Zeneca, Janssen, GSK, Novartis, Otsuka, Ben Parker Otsuka, J&J.