fetching data ... 
Background: Early diagnosis of connective tissue diseases (CTDs) is important to prevent irreversible organ damage and long-term morbidity. CTDs often present with heterogeneous and non-specific symptoms, making early recognition challenging in primary care. Conventional referral pathways are frequently associated with long waiting times and limited prioritisation. Digital fast-track referral models supported by eConsultation have emerged as a strategy to streamline access to rheumatology care and prioritise patients with suspected inflammatory disease, although real-world data specifically addressing CTDs remain limited.
Objectives: To describe access times and diagnostic outcomes of a digital eConsultation-based fast-track pathway for patients with suspected CTDs in a real-world tertiary care setting. Secondary objectives were to assess referral appropriateness according to predefined criteria and the diagnostic yield for clinically relevant inflammatory rheumatic diseases.
Methods: This retrospective service evaluation included all eConsultations referred to the fast-track CTD pathway between June 2021 and June 2025. The pathway enables primary care physicians to refer patients with suspected CTDs through structured electronic consultations, which are reviewed by a rheumatologist to determine the need and priority for face-to-face assessment. Primary outcomes were time to eConsultation response and time to face-to-face rheumatology assessment. Secondary outcomes included compliance with predefined referral criteria, need for ongoing rheumatology follow-up and final rheumatological diagnosis. Referral criteria were defined as the presence of at least two of the following features: inflammatory arthralgia, ANA titre >1:160, Raynaud phenomenon, mucocutaneous dryness, rash, aphthae, headaches, purpura or fever. Clinically relevant inflammatory disease was defined as a final diagnosis of connective tissue diseases or other inflammatory rheumatic diseases. CTDs included systemic lupus erythematosus, systemic sclerosis, Sjögren’s syndrome, inflammatory myopathies, undifferentiated connective tissue disease, Behçet’s disease and systemic vasculitis. Other inflammatory rheumatic diseases included inflammatory arthritis, spondyloarthritis, antiphospholipid syndrome and sarcoidosis.
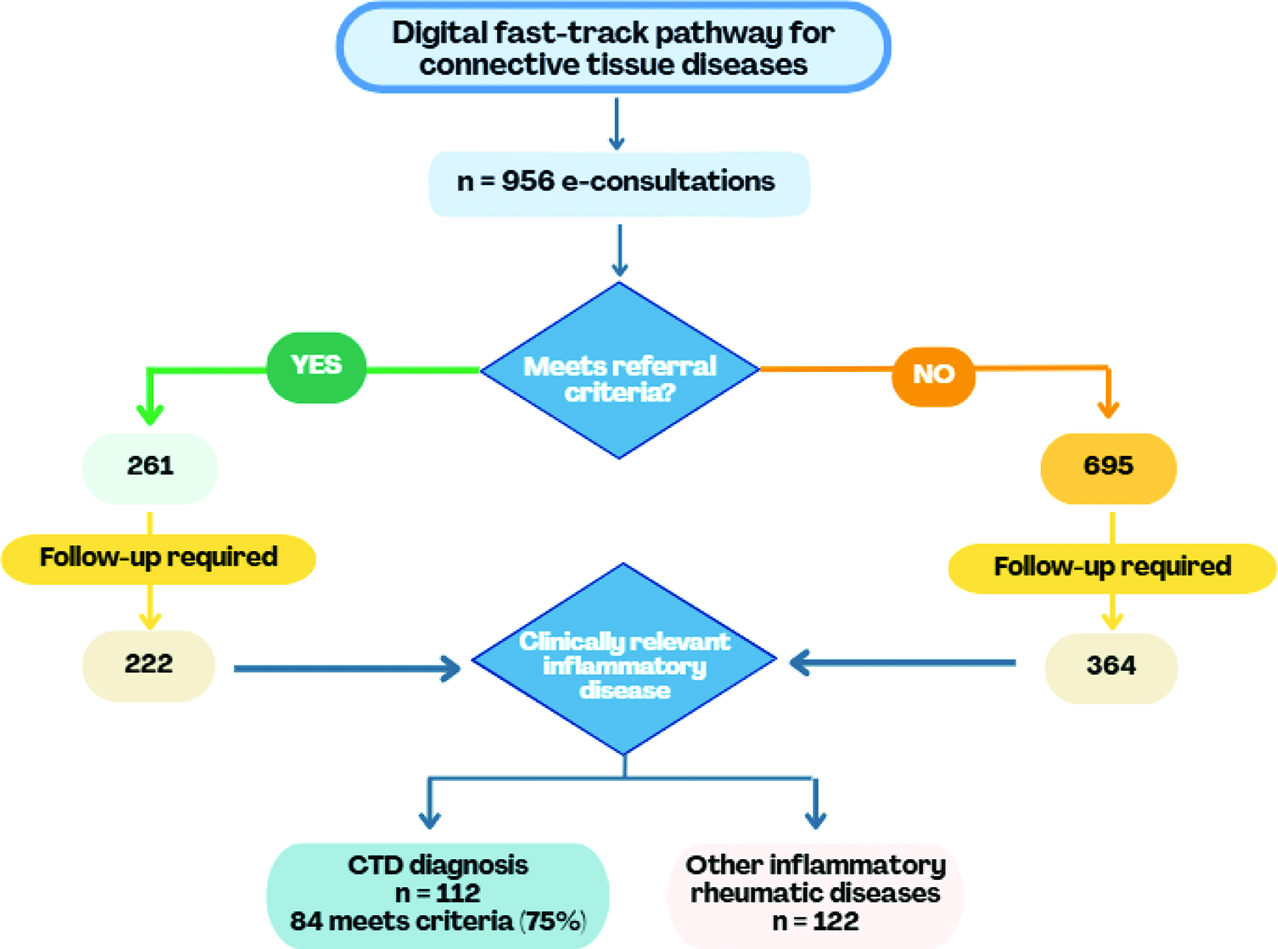
Results: A total of 956 eConsultations were analysed, with a progressive increase in referral volume over the four-year period. Mean eConsultation response time remained stable at approximately 5 days despite increasing demand. Median time to face-to-face rheumatology assessment was 30 days, with prioritisation according to clinical urgency. Patients were predominantly female (female-to-male ratio 3.6:1), and most were aged between 50 and 70 years. Overall compliance with predefined referral criteria was low, with only 27.3% of referrals fulfilling at least two criteria. Ongoing rheumatology follow-up was required in 61.6% of patients. Among those followed, 40% were diagnosed with clinically relevant inflammatory disease, including 19.1% with CTDs and 20.8% with other inflammatory rheumatic diseases. Among patients ultimately diagnosed with CTD, 75% fulfilled referral criteria at the time of eConsultation, while 25% were diagnosed despite not meeting predefined criteria (Figure 1).
Conclusions: In a real-world tertiary care setting, a digital eConsultation-based fast-track pathway facilitated prioritised access to rheumatology assessment and identified a substantial proportion of patients with clinically relevant inflammatory disease. The pathway effectively captured most CTD cases meeting referral criteria, while also identifying a relevant minority of patients who would have been missed using strict criteria alone. Low compliance with referral criteria highlights the need for targeted educational interventions in primary care to improve referral quality and optimise pathway efficiency. These findings support the implementation of scalable digital triage models to optimise access to rheumatology care and improve early CTD detection within high-demand healthcare systems.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.