fetching data ... 
Background: Functional limitation and physical activity routines are central components in the assessment of inflammatory rheumatic diseases such as rheumatoid arthritis (RA) and psoriatic arthritis (PsA). In routine clinical practice, multiple patient-reported outcome measures (PROMs) are frequently collected; however, it remains unclear which functional and physical activity domains are most informative with respect to the different diseases. This is especially relevant in daily practice, where improved insight into patient-reported functional limitations and quality-of-life impairments may reveal important aspects of disease burden that are often overlooked by routine clinical disease activity indices.
Objectives: To investigate, which categories of patient-reported function and physical activity behavior most effectively distinguish healthy individuals (HC) from patients with RA and PsA, and which items and domains are most informative.
Methods: For this cross-sectional study, RA (ACR/EULAR 2010) and PsA (CASPAR) patients were recruited from the Internal Medicine 3 outpatient clinics at Universitätsklinikum Erlangen, Germany, and HC over social networks (Ethics #357_20B). Disease activity was assessed using the Disease-Activity-Score-28 (DAS28-CRP) in RA and the Disease Activity in Psoriatic Arthritis (DAPSA) score in PsA. All participants completed the following PROMs: Disabilities of the Arm, Shoulder and Hand questionnaire (DASH), International Physical Activity Questionnaire (IPAQ), Michigan Hand Outcomes Questionnaire (MHQ), Physical Activity-related Health Competence scale (PAHCO), Score for the Assessment and Quantification of Chronic Rheumatic Affections of the Hands (SACRAH), 36-Item Short Form Health Survey (SF-36), and Tampa Scale for Kinesiophobia (TSK). A total of 274 numerical variables reflecting single components of all collected PROMs were derived, normalized and we used supervised machine learning model (Extreme Gradient Boosting (XGBoost), Decision Tree, Random Forest, logistic regression, support vector machine, k-nearest neighbors.) for binary classification of HC vs RA, HC vs PsA, and RA vs PsA. Model evaluation was performed using stratified cross-validation. In addition, a stratified 75/25 train–test split was used for visualization of confusion matrices. Model performance was assessed using classification accuracy and macro-averaged F1 score. Hyperparameters for tree-based models were optimized empirically, and the reported results correspond to the best-performing configurations. To identify the most informative non-clinical domains, feature selection techniques including SelectKBest and recursive feature elimination were applied. Feature relevance was further quantified using out-of-fold permutation importance analysis.
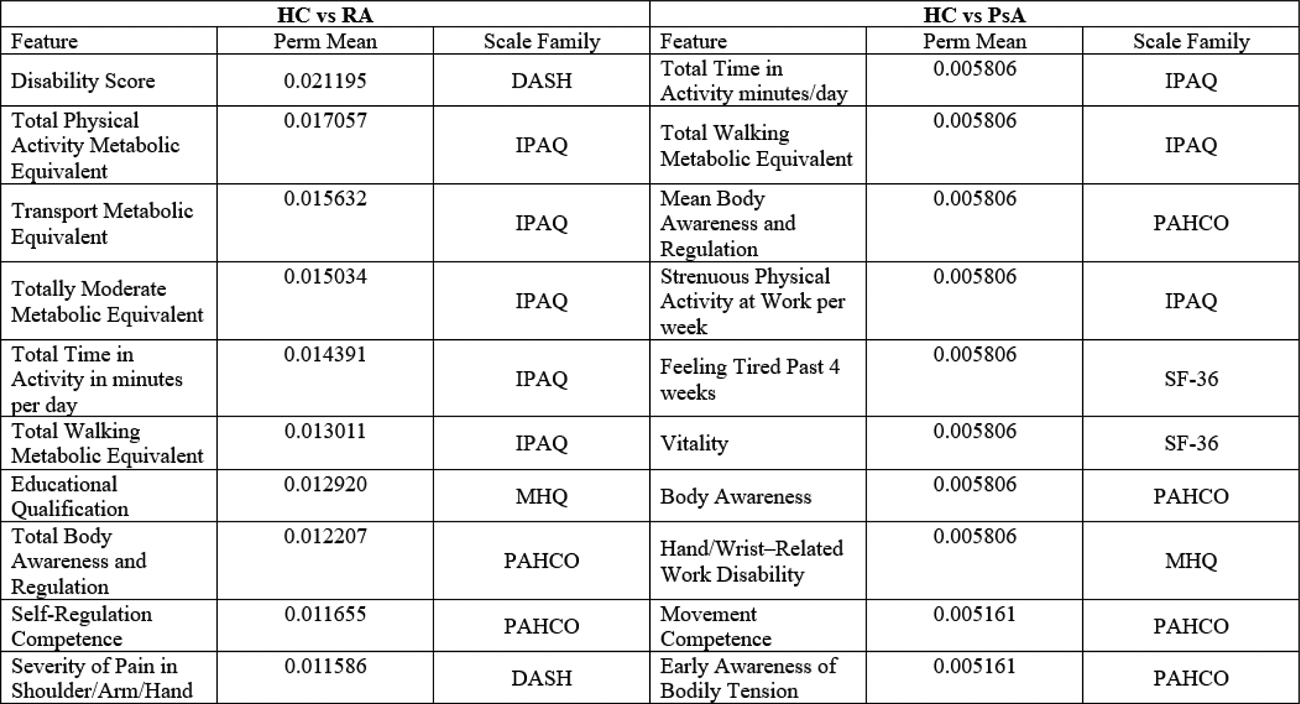
Results: For this analysis 224 participants were included (HC: n=75, age 45.8 (18.7) years, 40/35 f/m; RA: n=73, age 53.9 (14.1) years, 49/24 f/m; PsA: n=76, age 52.0 (14.3) years, 39/37 f/m). At the day of data collection patients showed low to moderate disease activity (RA: DAS28-CRP 2.56 (0.88); PsA: DAPSA, 10.18 (7.13)). Across all binary classification, the XGBoost model for HC vs RA achieved the best accuracy with 0.865, followed by HC vs PsA (accuracy= 0.711). The Decision Tree model achieved a similar accuracy for HC vs RA, and HC vs PsA, and the best accuracy of 0.526 for RA vs PsA (Figure 1). The best features for the classification of HC vs RA, predominantly included items of the IPAQ, DASH and PAHCO, with the DASH subscale of Disability as the most discriminative feature, followed by the IPAQ subscale of Total and Transport (walking/cycling) Metabolic Equivalent (MET). For the PsA vs HC comparison eight of the IPAQ, SF-36 and PAHCO subscales were the most informative features (Table 1).
Conclusions: Patient-reported outcomes measuring function and physical activity effectively distinguished HC from patients with inflammatory arthritis. In RA, discrimination was mainly driven by impaired hand function (DASH) and reduced daily physical activity (IPAQ). In PsA, time spent in transport-related physical activity, SF-36 vitality subscales and PAHCO subscales related to body awareness and self-regulation were particularly informative. RA and PsA could not be reliably differentiated by the applied methods, reflecting substantial overlap in patient-reported disease burden at low to moderate disease activity. This analysis underscores the value of targeted, item-level analysis of comprehensive PROMs to capture the most affected quality-of-life domains. This approach supports a more focused, patient-centered use of PROMs and highlights the need for tailored physical activity interventions and education to promote effective self-regulated physical activity.
The confusion matrices illustrates the binary classification performance of the XGBoost and Decision Tree models.
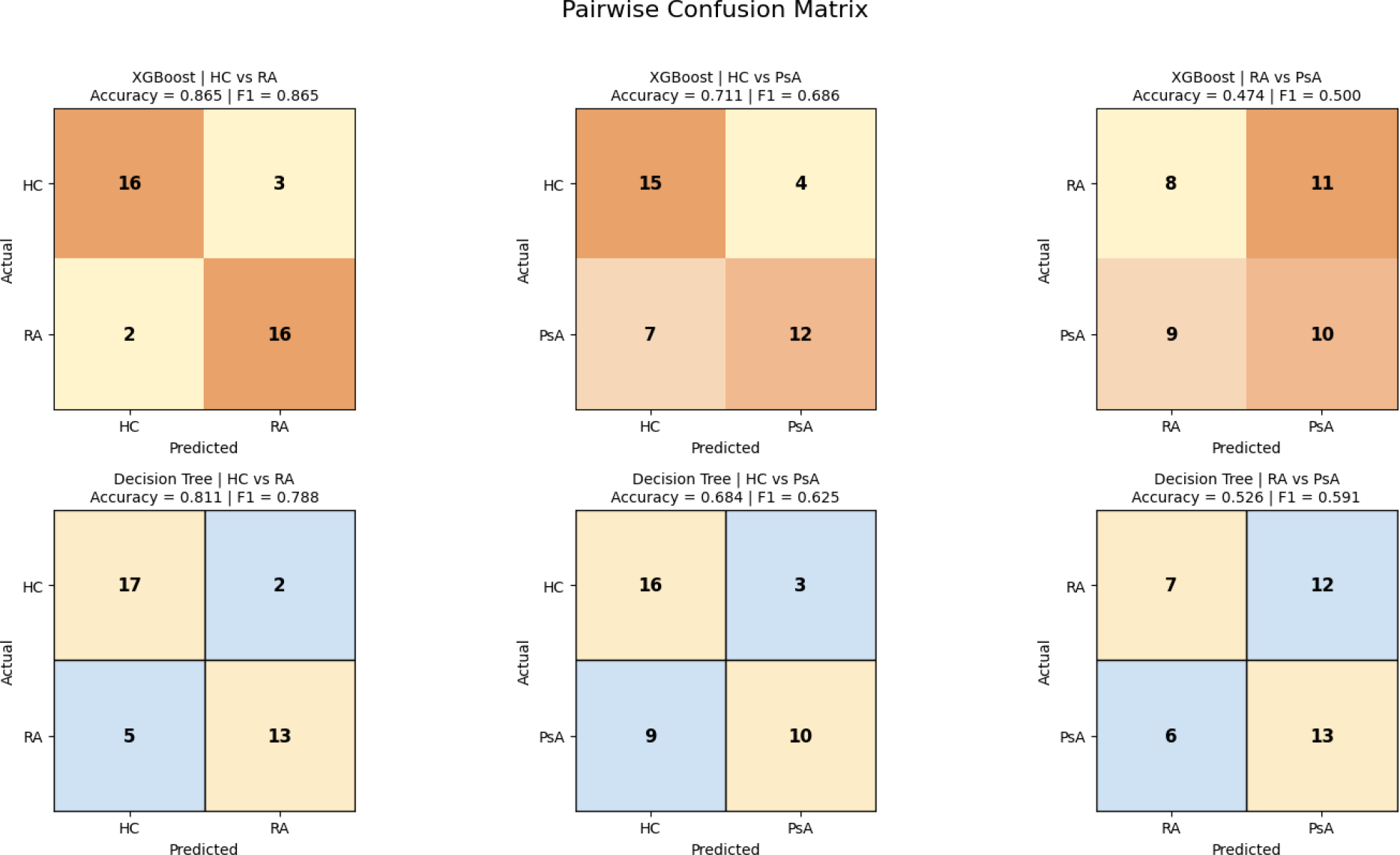
Table 1. Feature ranking by binary comparison based on out-of-fold permutation importance.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.