fetching data ... 
Background: Familial Mediterranean Fever (FMF) is a hereditary autoinflammatory disorder characterized by recurrent fever episodes, serositis, arthritis, and erysipelas-like erythema. Mutations in the MEFV gene, particularly in exon 10, are strongly associated with FMF, contributing to its clinical heterogeneity. While colchicine remains the cornerstone treatment, its efficacy varies depending on genetic mutations. Patients with inadequate responses or intolerance often require IL-1 inhibitors, such as anakinra or canakinumab, which are effective but costly. Recent advances in next-generation sequencing (NGS) have highlighted the presence of other autoinflammatory syndromes in FMF patients, particularly in those with atypical presentations or MEFV-negative status and most of them are more responsive to IL-1 inhibitors rather than colchicine. The influence of MEFV mutation status on treatment response and safety profiles of colchicine and IL-1 inhibitors remains incompletely defined. Understanding the impact of MEFV mutations on treatment efficacy, safety, and clinical outcomes is critical to optimizing patient management.
Objectives: This study aimed to assess the influence of MEFV mutations on colchicine efficacy and safety, as well as the need for IL-1 inhibitors in FMF patients. Additionally, it explored clinical and laboratory changes after most effective FMF treatment, comparing MEFV-positive and MEFV-negative patients. The goal was to identify diagnostic and therapeutic challenges, particularly in atypical cases, and provide insights into improving personalized treatment strategies.
Methods: This cross-sectional single-center study included 500 patients with FMF followed between April 2020 and October 2025. Patients were stratified according to MEFV mutation status into mutation-positive (n=412) and mutation-negative (n=88) groups. MEFV-positive patients included those with exon 10 mutations (homozygous or heterozygous), while MEFV-negative patients had no pathogenic mutations or only benign mutations (e.g., R202Q, E148Q). Demographic features, treatment characteristics, and outcomes were extracted from medical records. Colchicine efficacy, need for anti-IL1 or other biologic therapy, and treatment-related adverse events were assessed. Comparative analyses were performed between groups to evaluate differences in disease phenotype, treatment response, and safety.
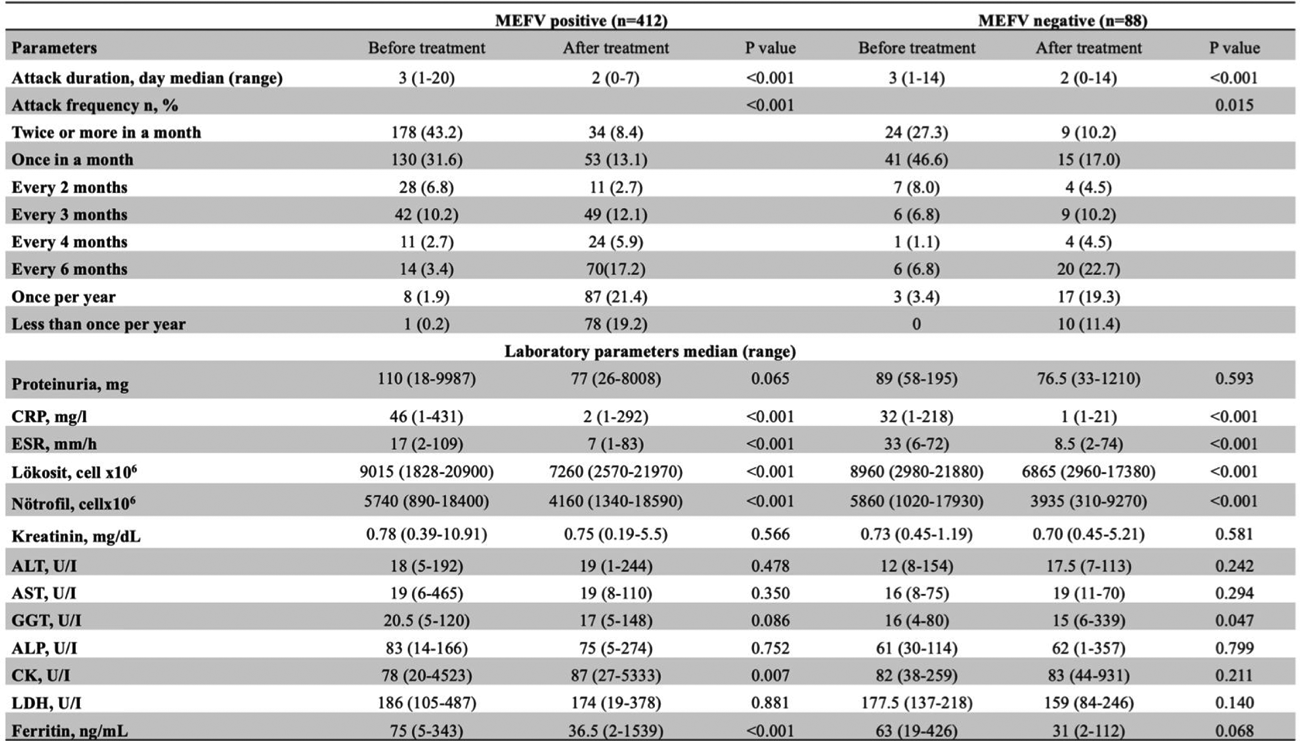
Results: Demographic data and treatment characteristics of both MEFV positive and negative groups were given in Table 1. Patients with MEFV mutations were diagnosed at a significantly younger age compared with mutation-negative individuals (median 14 vs 26 years) and experienced shorter diagnostic delay. Colchicine was administered to all patients and led to significant reductions in attack frequency and inflammatory markers in both groups (p<0.05 for all acute phase reactants parameters). However, the magnitude of inflammation control regarding decrese in CRP, ESR, neutrophilia and serum ferritin levels was greater among MEFV -positive patients (p<0.001 in all). Details of laboratory paramaters were given in Table 2. Attack duration and frequency decresed after effective treatment in both groups but decrease in attack frequency was more prominent in MEFV positive group (p value <0.001 vs 0.015). Colchicine intolerance and partial response were similar between groups. Although not reached in significance level, the distribution of colchicine adverse events were different between groups. Hepatotoxicity was more common in MEFV positive group (26.0 vs 18.2%) while nause was more common in MEFV negative group (23.6 vs 31.8%). Anakinra and canakinumab were effective in controlling disease activity in both groups, although inadequate response to anakinra was observed more frequently among MEFV -negative patients (17.5 vs 33.3%, respectively). Canakinumab demonstrated sustained efficacy and favorable tolerability regardless of genotype.
Conclusions: The study highlights clinical and therapeutic differences between MEFV-positive and MEFV-negative FMF patients. MEFV-negative patients present diagnostic challenges due to atypical features and prolonged diagnostic timelines, often requiring more advanced genetic testing and tailored treatment strategies. While colchicine effectively reduces attack severity and inflammation in both groups, MEFV-positive patients demonstrated superior inflammation control. The more effective inflammation control observed in MEFV-positive patients support the potential of colchicine to regulate pyrin-mediated and IL-1 driven inflammation, particularly in typical FMF cases with exon 10 mutations. The differences in adverse event profiles may be interpreted as the differences in metabolism of colchicine in both groups and additinal liver involvement and particular tendency for elevated transaminases in typical FMF cases which we observed as hepatotoxicity. Implementing NGS-based exome sequencing and broader autoinflammatory panels can refine diagnoses, particularly in MEFV-negative or colchicine-refractory cases and help to identify patients with overlapping additional autoinflammatory diseases or other undiagnosed hereditary peroidc fever syndromes responding anti-IL1 blockers, and colchicine in some. This approach enables more precise, cost-effective management, and improved patient outcomes for these special subgroup. Future research should focus on integrating genetic findings with clinical phenotypes to develop personalized treatment strategies.
Table 1. Baseline demographics, diagnosis process and treatment history in patients according to MEFV positivity
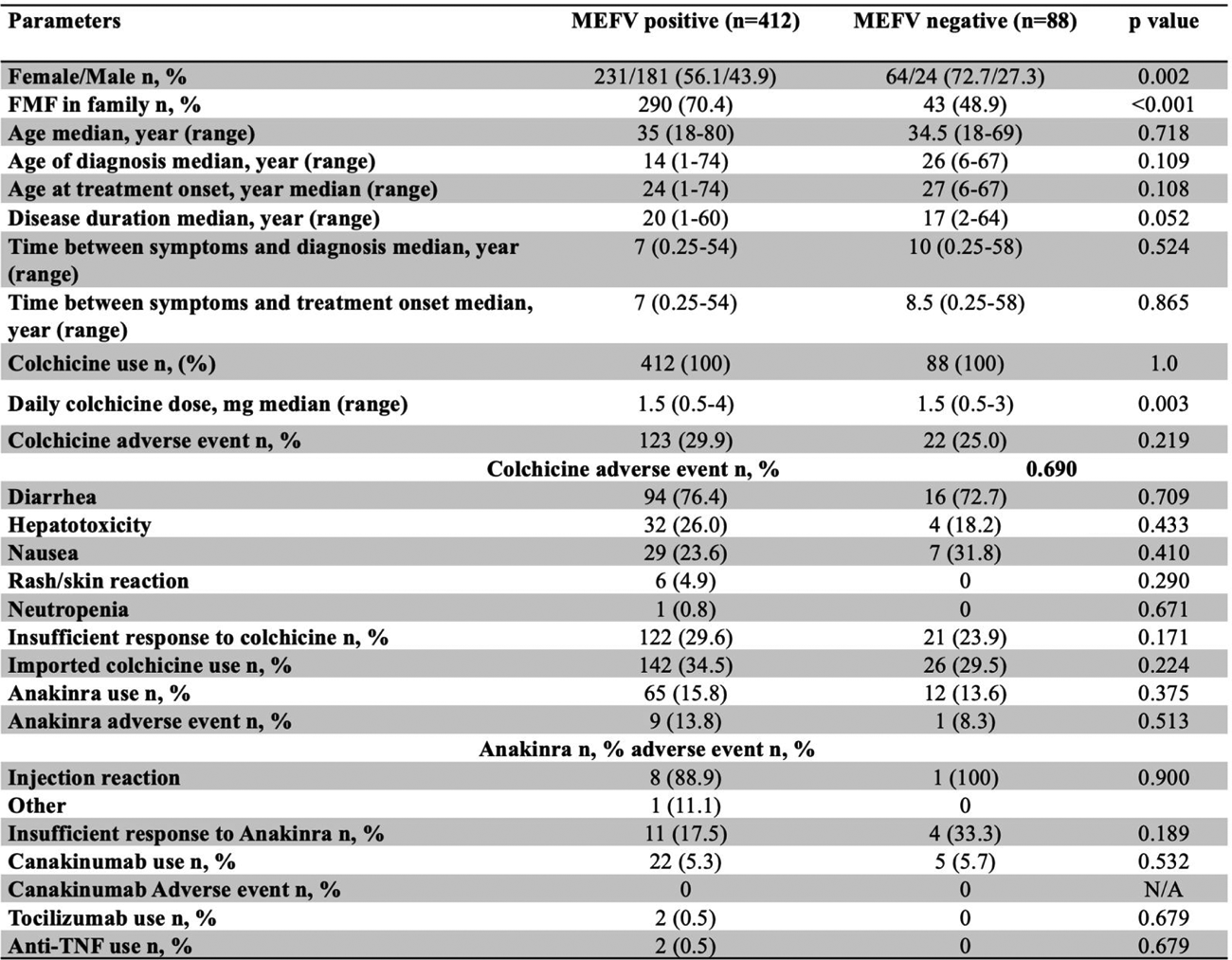
Table 2. Changes in attack characteristics and laboratory parameters after treatment according to MEFV positivity
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.