fetching data ... 
Background: Familial Mediterranean Fever (FMF) is a hereditary autoinflammatory disorder characterized by recurrent febrile episodes and serosal inflammation. Management of FMF requires lifelong colchicine therapy, and no curative treatment is currently available. Living with a chronic, relapsing disease that necessitates continuous medication throughout life may be associated with an increased psychological burden, and adverse mental health outcomes, such as depression and suicidal behavior. In this context, colchicine may emerge as a suicide method, and its toxicity deserves careful attention. To date, intentional colchicine overdose resulting in completed suicide among patients with FMF has been limited to case reports, indicating an unmet need for more comprehensive evaluation
.
Objectives: This study aimed to evaluate colchicine-related fatal toxicity in FMF patients, with a focus on demographic characteristics, clinical course, post-mortem histopathological findings, and psychosocial background following intentional overdose.
Methods: A retrospective observational investigation of FMF patients who died by suicide following intentional colchicine overdose was conducted. The records of the Council of Forensic Medicine, Ministry of Justice were screened for eligible patients. For each patient identified, data were collected on ingested colchicine dose, timing of presentation, clinical manifestations of toxicity and in-hospital course, including all the events occurring between emergency department admission and intensive care unit transfer. Laboratory findings and organ involvement were recorded. Histopathological data were obtained from post-mortem examinations when available. Psychosocial information, including documented psychiatric diagnoses, prior disclosure of suicidal intent and contextual factors surrounding the suicide event, was extracted from forensic reports, medical files and family interviews. Data were explored and reported using descriptive methods.
Results: The study included 15 FMF patients who died by suicide following intentional colchicine overdose; 87% were female. The mean age was 28.4 (±16.85) years. The mean ingested colchicine dose was 54.5 (±31.79) mg. Eight patients (53%) were single. At least one comorbidity was documented in 7 patients (47%). Only 1 patient was under regular psychiatric follow-up (Table 1). 3 patients (20%) had at least one child at the time of intentional overdose. Prior disclosure of suicidal intent was documented in 3 patients (20%): 2 patients disclosed suicidal thoughts to a close friend and 1 patient to a partner before the attempt. Reported reasons for suicide included family-related conflict (27%), FMF-related pain (27%), romantic relationship problems (20%), gender identity-related distress (13%), bereavement following the death of a child (7%) and exacerbation of major depressive disorder (7%).
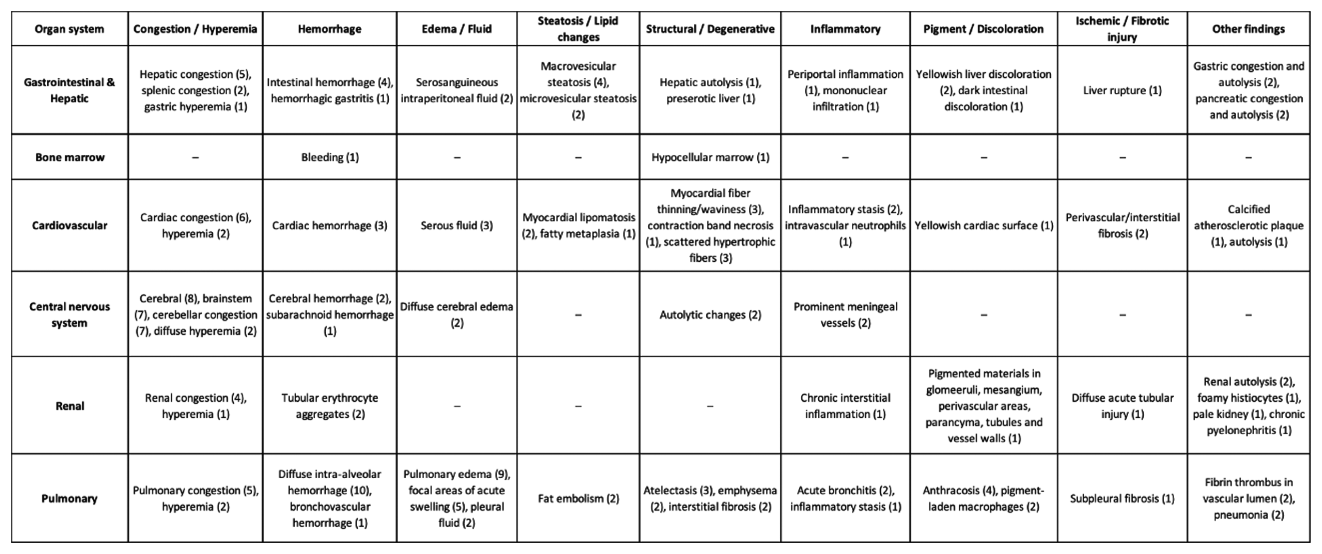
Gastrointestinal symptoms such as nausea and vomiting were the most frequent initial presentation, observed in 27% of patients. Less commonly, patients presented with cardiac arrest, hypotension, multiorgan failure, peripheral neuropathy, and tremor. The mean time from ingestion to emergency department presentation was 11.9 (±15.28) hours. Clinical deterioration was rapid; the mean time from ingestion to intubation was 1.63 (±0.91) days, and the mean time to death was 5.18 (±4.47) days. Post-mortem examinations revealed multisystem involvement (Table 2). Pulmonary findings were predominant, including diffuse intra-alveolar hemorrhage (67%), pulmonary edema (60%). Hepatic pathology frequently showed congestion (33%), macrovesicular steatosis (27%). Cardiovascular findings comprised widespread congestion (40%) and findings compatible with myocardial infarction (20%). Renal pathology showed congestion (27%) and amyloid deposition. Central nervous system findings were dominated by cerebral and brainstem congestion (53%).
Conclusions: Colchicine overdose represents a highly lethal suicide method in FMF patients, with rapid clinical deterioration and progression to multiorgan failure in the absence of a specific antidote, most commonly observed in young female patients. Despite the prior disclosure of the suicide intent in 3 (20%) patients, regular psychiatric follow-up was notably limited, with only 1 (7%) patient. Considering these patients disclosed suicidal intent to individuals outside the family, strengthening psychosocial awareness and communication within families and broader social networks may play a critical role in preventing fatal outcomes. Among the reasons for suicidal behaviour, family-related conflict and FMF-related pain emerged as frequently reported precipitating factors, emphasizing the paramount importance of raising awareness among family members of FMF patients and providing adequate symptom control. Gender identity-related distress represented a prominent contributing factor but remains underrecognized in routine clinical practice. In-hospital courses of all patients were consistent with the classical progression of colchicine toxicity, the mean time to death corresponding to phase 2, also known as the multi-organ failure phase. Post-mortem analyses demonstrated widespread organ damage. In conclusion, these findings highlight the importance of close and continuous mental health monitoring in FMF patients, particularly those with persistent pain or psychosocial stressors. Given the lifelong use of colchicine in this population, limiting access to large quantities of colchicine is crucial to reduce the risk of fatal outcomes, specifically for patients at high risk of intentional overdose.
Table 1.
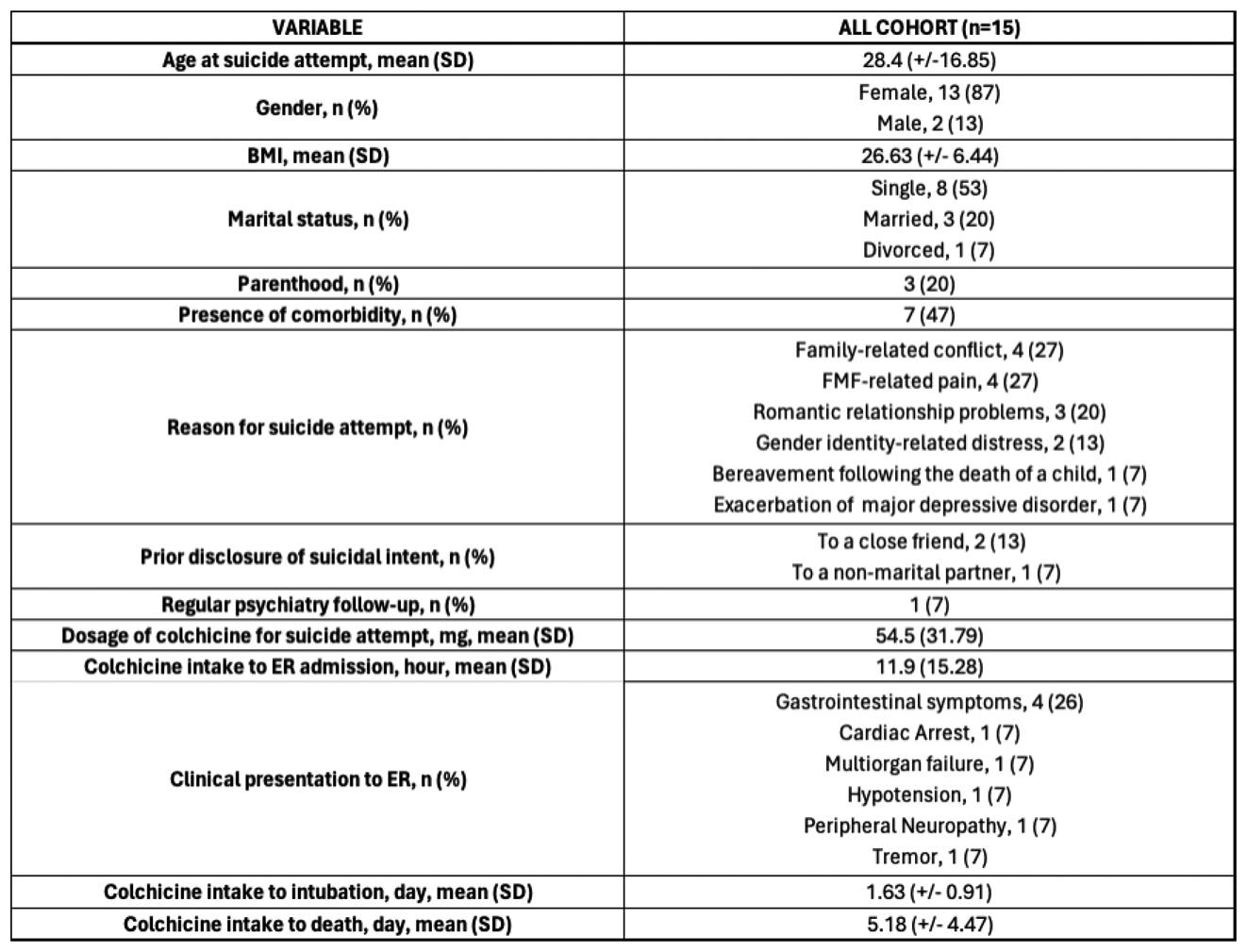
Table 2.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.