fetching data ... 
Background: Familial Mediterranean Fever (FMF) is a prototypical autoinflammatory disease characterized by recurrent episodes of fever, serositis, arthritis, and erysipelas-like erythema, predominantly affecting populations of Turkish, Armenian, Arab, and Jewish descent. The condition is closely associated with mutations in the MEFV gene of chromosome 16, particularly in exon 10, which plays a critical role in encoding pyrin, a protein involved in inflammasome regulation. Nevertheless, a substantial proportion of clinically diagnosed FMF patients lack identifiable MEFV mutations, posing diagnostic and therapeutic challenges. The presence of genetic variability introduces clinical heterogeneity, complicating the diagnostic process in some cases. Moreover, atypical presentations in patients without MEFV mutations, or those with no or partial colchicine responses, raise the possibility of other underlying autoinflammatory syndromes. Advances in next-generation sequencing (NGS) exanded the identification of FMF and other autoinflammatory diseases, revealing shared phenotypes such as fever, acute-phase response elevation, and periodic inflammatory episodes alongside distinct clinical features. On this context, the data comparing clinical characteristics, disease manifestations, and diagnostic complexity between genetically defined and mutation-negative FMF populations remain limited.
Objectives: To compare clinical features and disease characteristics between MEFV -positive and MEFV -negative patients diagnosed with FMF and to identify distinguishing features that may facilitate earlier diagnosis and improved disease management.
Methods: This cross-sectional study included FMF patients from a tertiary rheumatology center under regular follow-up between April 2020 and October 2025. Data were collected through direct interviews and patient records, encompassing demographics, clinical manifestations, genetic testing(MEFV mutations). Patients with typical exon 10 mutations(homozygous or heterozygous) were classified as MEFV-positive, while those without mutations or with benign variants (e.g.R202Q and E148Q in exon 2) were categorized as MEFV-negative. Demographic characteristics, clinical manifestations, attack patterns, and disease-related complications were retrospectively analyzed. Classical FMF manifestations (fever, serositis, arthritis, etc) as well as atypical features (e.g., prolonged attacks, urticaria, pharyngitis, lymphadenopathy, oral apthae, etc) were systematically evaluated. Statistical comparisons were performed to identify differences between groups.
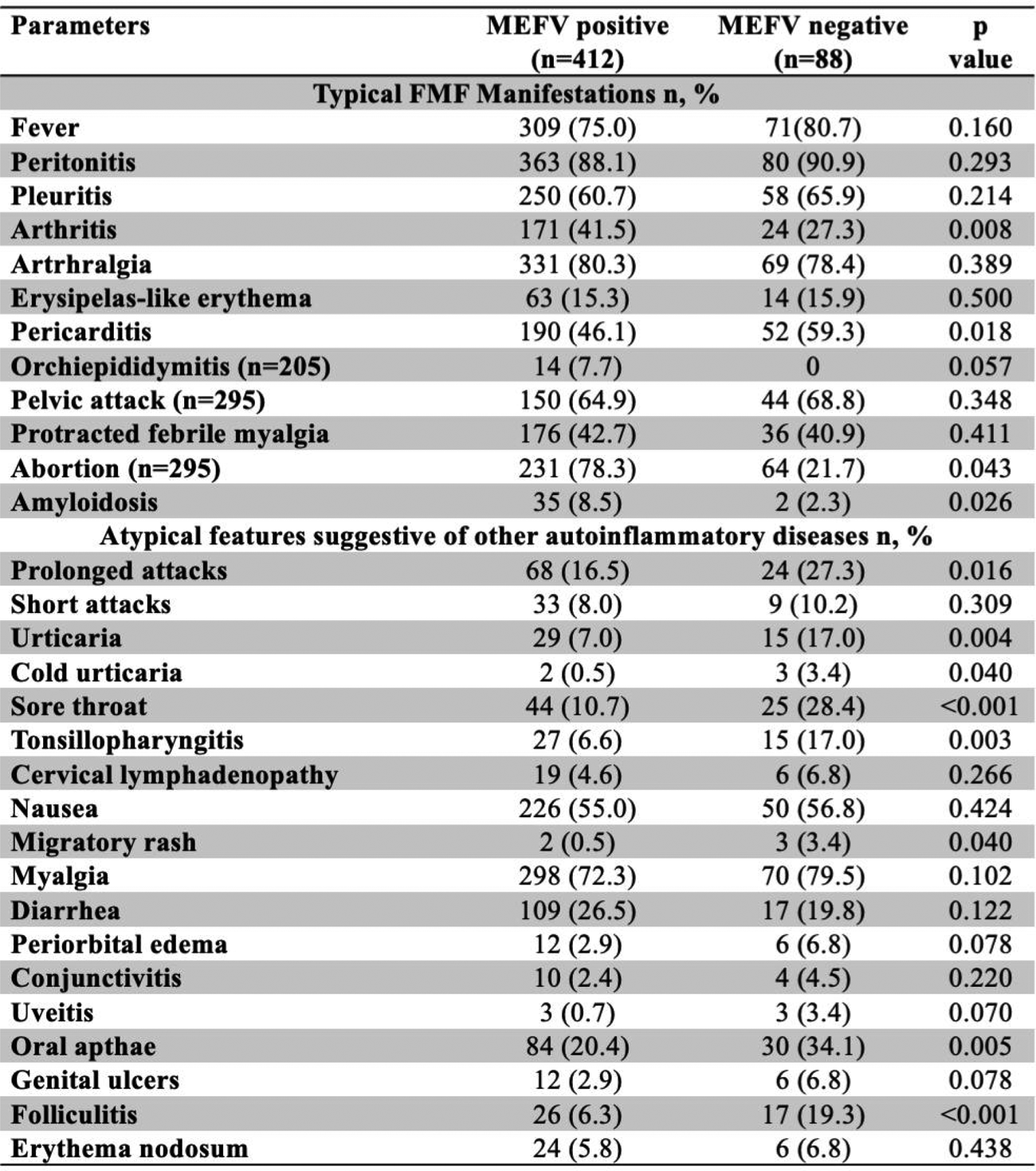
Results: Among the 500 patients included, 412(82.4%) carried at least one pathogenic MEFV mutation, while 88(17.6%) were mutation-negative. The mutation-negative group had a significantly higher median age at diagnosis (26 vs 14 years, p=0.021) and a longer diagnostic delay(10 vs 5 years, p=0.043) as given detailly in Table 1. Typical FMF manifestations such as fever, peritonitis, pleuritis, and arthritis were observed at comparable frequencies between groups(Table 2). However, several atypical features were significantly more frequent in the MEFV -negative group, including prolonged attacks, urticarial eruptions, pharyngitis, tonsillitis, and migratory rash (p<0.05 in all). Also, pericarditis was more ommon in MEFV -negative group(46.1 vs 59.3, p=0.03). Conversely, arthritis and amyloidosis were more prevalent in MEFV -positive patients. Laboratory analysis revealed higher inflammatory markers during attacks in both groups, while persistent subclinical inflammation outside attacks was more pronounced in MEFV -positive patients.
Conclusions: This large real-world cohort highlights the substantial clinical heterogeneity in FMF patients, particularly among without MEFV mutations. The typical FMF symptoms, such as fever and serositis, were common in both MEFV-positive and negative groups. However, while MEFV -positive patients exhibit more classical inflammatory patterns and higher amyloidosis risk consistent with FMF, MEFV -negative patients were more likely to present with atypical features such as urticaria, tonsillopharyngitis, and longer attack durations and heterogeneous presentations that may complicate diagnosis and management. These findings demonstrate that FMF patients without detectable MEFV mutations constitute a clinically distinct subgroup characterized by atypical inflammatory manifestations, and increased possibility to have overlapping phenotypes with other autoinflammatory diseases namely hereditary periodic fever syndromes like cold associated periodic syndrome, mevalonate kinase deficiency syndrome or TNF receptor assciated peridoic syndrome or even misdiagnoses of other autoinflammatory syndromes due to high frequency of FMF. On the other hand, pericarditis is the least expected serositis type in FMF and it was more common in MEFV-negative group, probably related with idiopathic recurrent pericarditis and other entities. Also, the extended diagnostic timelines in MEFV-negative patients reflect the challenges posed by atypical clinical presentations, often necessitating advanced diagnostic tools such as NGS and comprehensive autoinflammatory disease panels. Incorporating detailed phenotypic assessment alongside advanced analysis in selected cases may aid in identifying misdiagnosed or overlapping syndromes and refining diagnostic accuracy. Incorporating NGS and expanding the diagnostic spectrum to include other autoinflammatory syndromes may not only enhance the accuracy of FMF diagnoses, diagnose of but also optimize patient management. Such an approach is critical for improving clinical outcomes, minimizing diagnostic delays, and reducing healthcare costs. This study suggessts the need for a more nuanced understanding of FMF and its variants, ultimately contributing to the development of personalized treatment strategies.
Table 1. Demographics, diagnosis and attack characteristics according to MEFV positivity
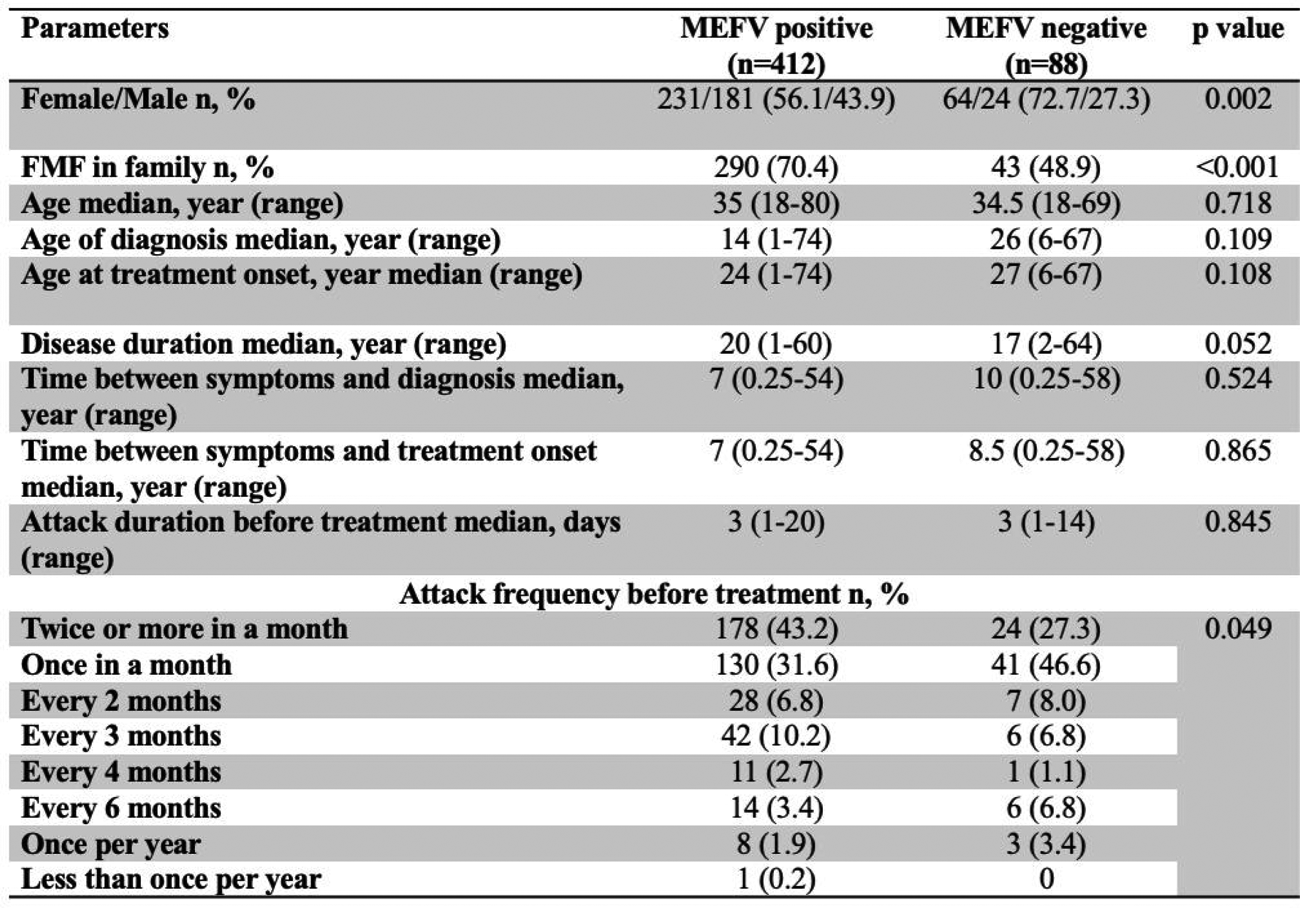
Table 2 . Clinical manifestations of patients according to MEFV positivity
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.