fetching data ... 
Background: Calcium pyrophosphate (CPP) deposition (CPPD) is a common crystal-induced arthropathy characterised by deposition within articular and fibrocartilaginous tissues, contributing to joint inflammation and degeneration. Ultrasound (US) plays a central role in CPPD diagnosis and assessment, as recognised by the 2023 ACR/EULAR classification criteria and EULAR imaging recommendations, due to its higher sensitivity compared with radiography. OMERACT has also developed and validated a US scoring system to identify and grade CPP crystal deposition and cartilage involvement.
Following the feasibility testing of deep learning–based CPPD grading on manually cropped US images with suboptimal clinical performance [1], we explored a more advanced approach based on semantic segmentation. This approach provides structured supervision by training the model to identify and label, pixel by pixel, anatomical structures such as crystal deposits or bone, generating reference masks for different tissues and enabling accurate mask reproduction
Objectives: To develop and evaluate an AI-based semantic segmentation approach for identification and grading of CPPD in ultrasound images of knee menisci.
Methods: A dataset of US images of the knee meniscus was created by the OMERACT US working group members and graded on a four-level scale (grades 0–3) by the facilitators according to the OMERACT scoring system. Regions of interest (including the meniscus and both bone profiles used as landmarks) were cropped from the original images and preprocessed using greyscale normalisation and resizing to 256 × 256 pixels.
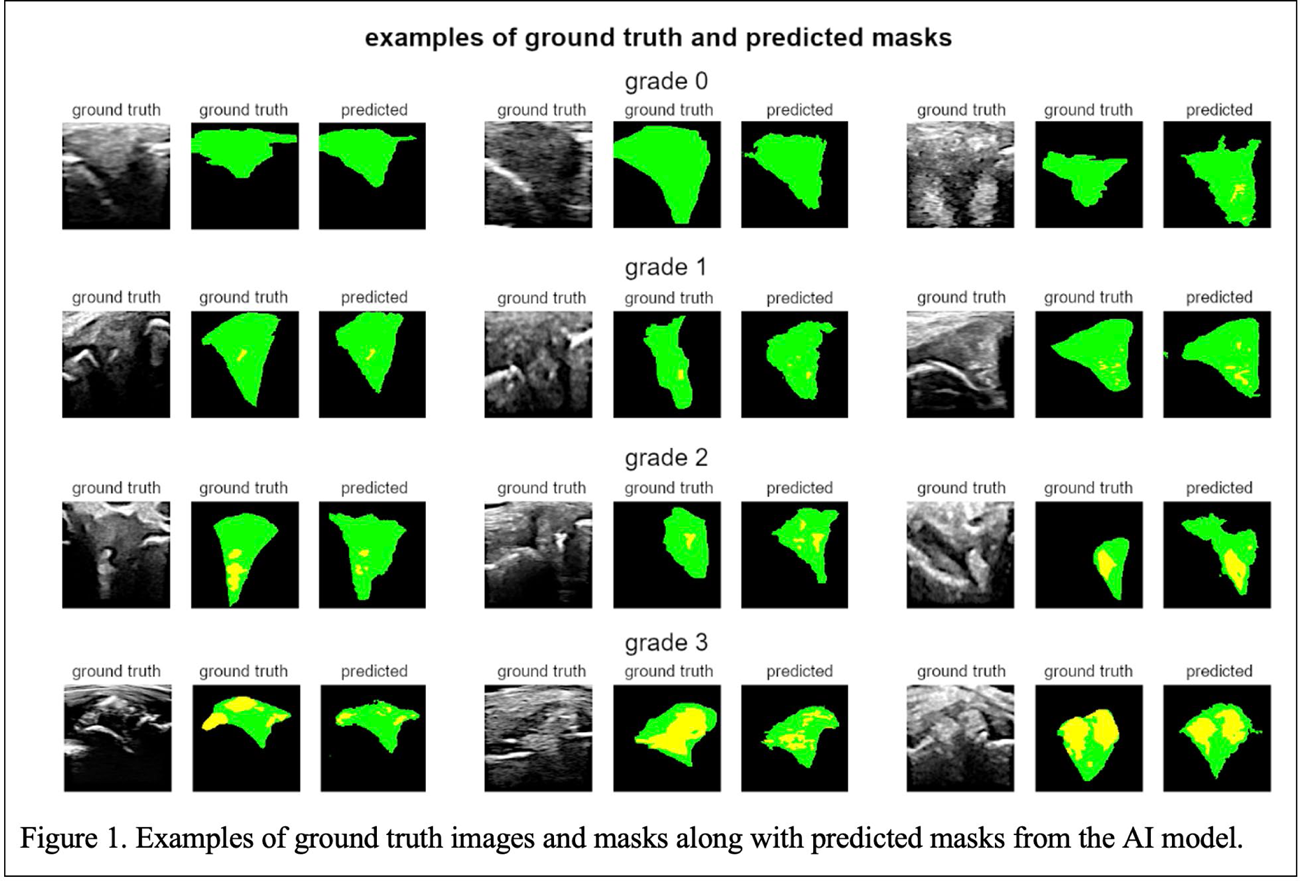
For semantic segmentation, experienced US operators performed manual labelling of the meniscus, CPP deposition, soft tissues and bone profiles at the pixel level that was used as ground truth (reference standard). The deep learning segmentation algorithm task was formulated to identify the following three items: background (including soft tissues, bone and under the bone area), meniscus, and crystal deposits (Figure 1).
Various convolutional neural network architectures used for medical image segmentation were evaluated either from scratch or using ImageNet-pretrained backbones. The dataset was randomly split by dedicated software into training (80%) and validation (20%) sets, preserving class distribution. Models were trained using combined dice loss and focal loss, promoting accurate mask overlap and enhanced learning of small crystal deposits. Data augmentation was applied during training.
Segmentation performance was evaluated on the validation set using the intersection over union (IoU), a metric that quantifies the spatial overlap between predicted segmentation masks and the corresponding reference masks for each tissue class. IoU values were computed at the image level and then averaged across all images to obtain mean IoU values for background, meniscus, and CPPD deposits.
To translate segmentation results into an interpretable measure (scoring of extent of deposition within the meniscus), an area ratio (AR) index was calculated for each image as the proportion of pixels corresponding to CPPD deposits relative to the total area of the meniscus plus deposits. Thus, the AR index provides a quantitative estimate of the extent of crystal deposition within the meniscus. Optimal AR thresholds for CPPD grading were derived using ground-truth segmentation masks from the complete dataset and were subsequently applied to AR values obtained from predicted masks to assign CPPD grades (0–3). Classification accuracy was calculated as the proportion of images in which the grade assigned using AR thresholds derived from predicted masks matched the ground truth.
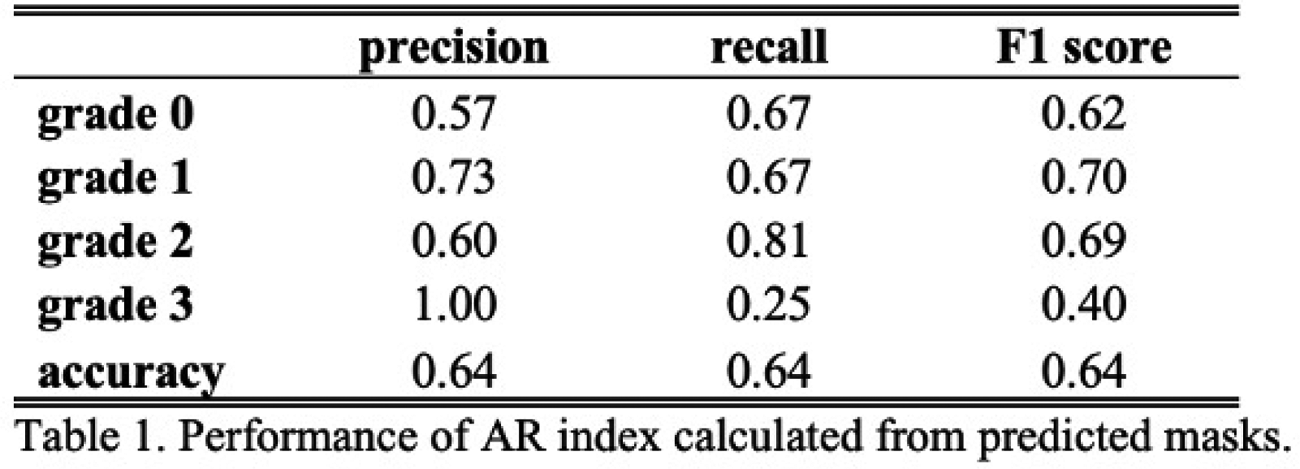
To further characterise grading performance, class-specific precision, recall and F1-score were calculated. Precision reflects the reliability of grade predictions by quantifying the proportion of correctly classified images among those predicted for a given grade, whereas recall reflects sensitivity by quantifying the proportion of correctly identified images among all true images of that grade. The F1 score represents the harmonic mean of precision and recall.
Results: A dataset of 279 images was analysed. Optimal AR thresholds were 0.0016 (corresponding to the grade 1 threshold), 0.0259 (corresponding to the grade 2 threshold), and 0.2009 (grade 3). This configuration achieved an overall accuracy of 0.82, with strong class-specific classification performance on ground-truth masks.
Among the evaluated models, the best-performing configuration was a LinkNet architecture with a pretrained ResNet34 backbone. Segmentation performance yielded mean intersection over union (IoU) values of 0.86 for background, 0.60 for meniscus, and 0.37 for CPPD deposits.
When the area ratio (AR) index was derived from predicted masks, accuracy in the validation set was 0.64, with class-specific performance summarised below (Table 1).
Conclusions: We explored AI-based segmentation for CPPD grading using the AR index. Although segmentation accuracy was limited (IoU = 0.37), the classification accuracy of 64% supports the continued development of this framework. Current performance, which did not exceed simpler non-segmentation approaches, likely stems from limited dataset size and morphological variability. Future research will focus on increasing image variability to refine these models for potential clinical integration.
REFERENCES: [1] DOI: 10.1016/j.ard.2025.05.306
Acknowledgments: NIL.
Disclosure of Interests: None declared.