fetching data ... 
Background: People living with arthritis were among the first to take on meaningful roles as partners in research, and their contributions have helped shape research priorities, study designs, outcome measures and more [1]. To date, these contributions have largely been described as involvement , whereby lived experience informs research but decision-making power typically remains with academic researchers. In contrast, studies led by patients and public—where individuals with lived experience hold final decision-making power [2] —remain poorly understood. As interest in this area grows, clearer definitions of what patient- and public-led research entails are needed. Without such clarity, leadership risks being conflated with involvement, limiting the ability to intentionally design, resource, and evaluate research that aspires to be patient- and public-led.
Objectives: To understand how patient- and public-led research (PPLR) is defined and practiced in health research.
Methods: Our scoping review was guided by Arksey and O’Malley’s framework (2005)[3] and reported in accordance with PRISMA-ScR [4]. A comprehensive search of health research databases and key grey literature sources was conducted. Included studies were published in English and described how patients and public held decision-making power across various research roles and tasks, including initiating research or conducting investigation. These standardized roles and tasks were described using the Contributor Role Taxonomy (CRediT)[5]. Studies that described patient and public governance of the research process or ownership of research products were also included. Through iterative team discussions and abductive analytic processes, a typology extending beyond standardized roles and tasks emerged.
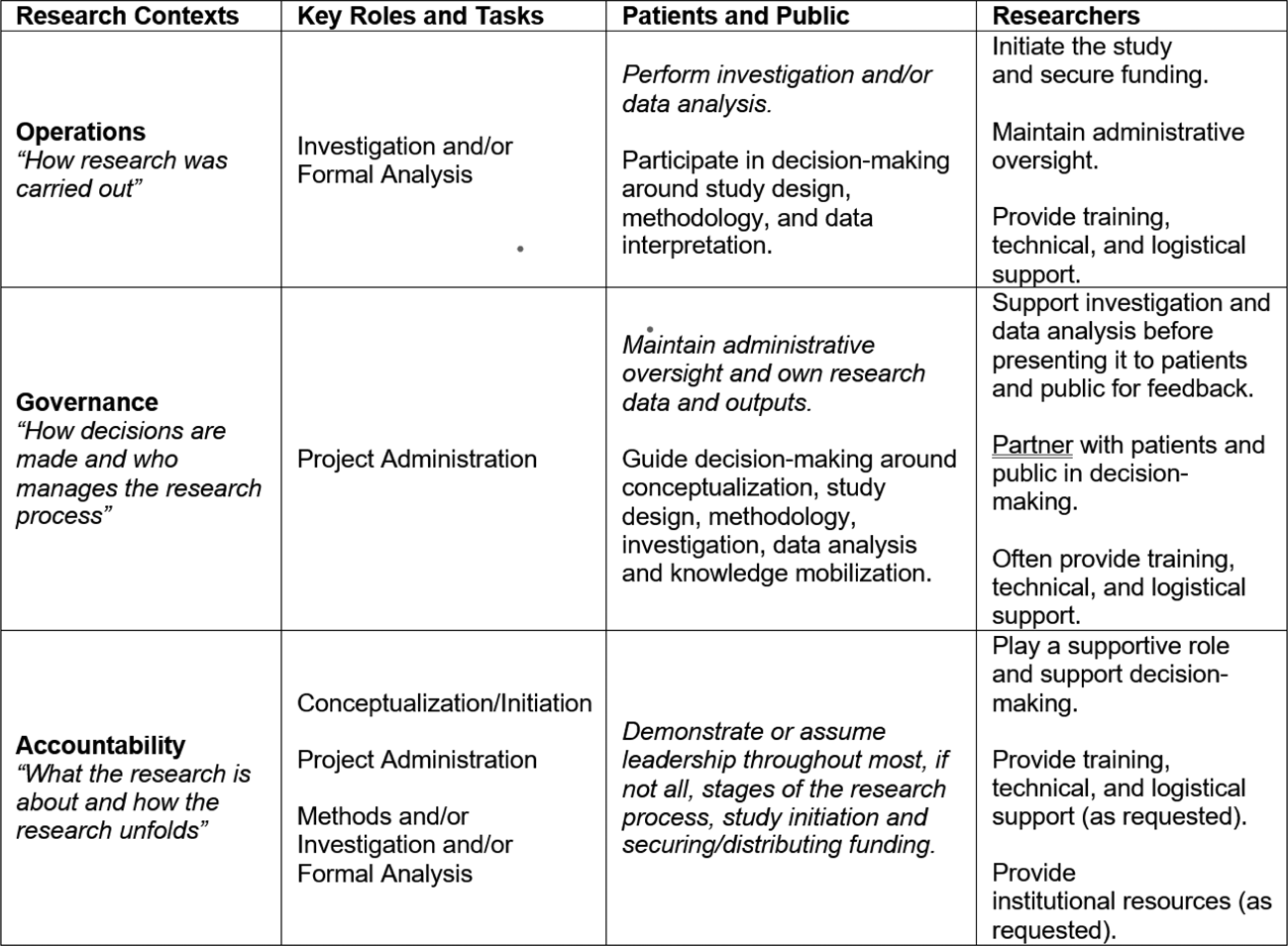
Results: From 4,723 records, 68 articles describing 62 studies met inclusion criteria. Although terminology varied (e.g., consumer-led, user-led, Indigenous-led), only 14 (23%) of studies explicitly defined PPLR. Included studies spanned a wide range of health topics, from maternal health to water contamination, and were conducted across all six continents. The majority, 53 studies (85%) were non-experimental (i.e., observational), while five studies (8%) involved self-experimentation, in which individuals designed and conducted experiments on themselves. Figure 1 illustrates the level of patient and public involvement across CRediT roles and tasks, revealing patterns and variation in decision-making power across the research process. Our analysis further revealed three contexts that describe how PPLR was conceptualized (Table 1): Operations (31 studies), describing how research is carried out; Governance (3 studies), describing how decisions are made and who manages the research project; and Accountability (24 studies), describing what the research is about and how it unfolds. Our results indicate that patients and public exercised diverse forms of power beyond decision - making , such as shaping research agendas and determining what forms of knowledge were included in the research study. Moreover, their experiential and intellectual contributions were comparable to those of principal investigators, particularly in study conceptualization and administration. This included how patients or public applied for, managed, or made decisions regarding funding allocation, which was reported by 23 (37%) studies.
Conclusions: Although lived experience has long been integral to RMD research, this review highlights that patient- and public-led research has been more clearly articulated in other areas of health research. By delineating distinct PPLR contexts, this review positions RMD research to build upon existing work. In doing so, it provides a foundation for conceptual clarity, and the rigorous design, resourcing, and evaluation of future patient- and public-led research in RMD.
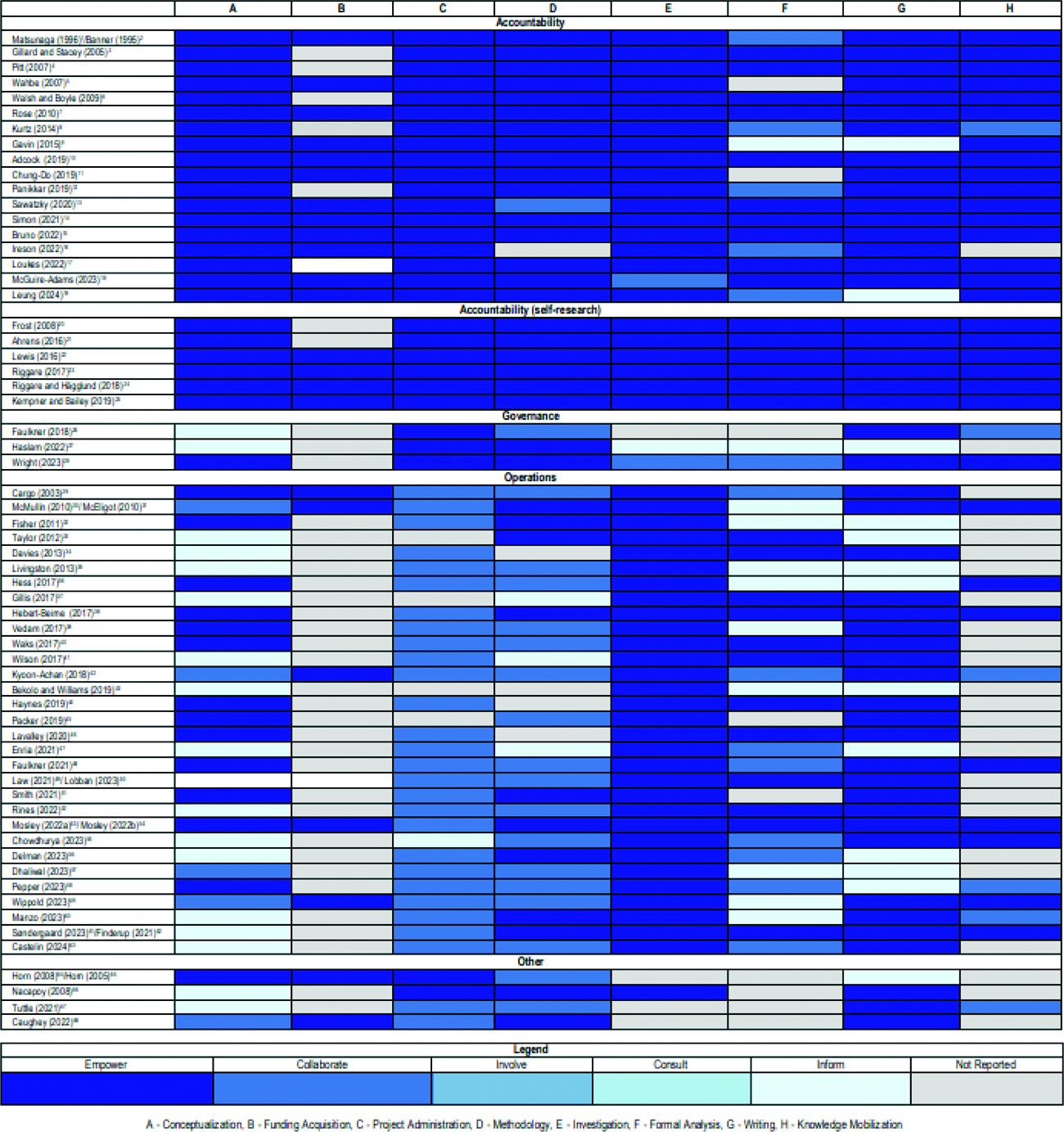
Table 1.
REFERENCES: [1] de Wit, M., Abma, T., Koelewijn-van Loon, M., Collins, S., & Kirwan, J. (2013). Involving patient research partners has a significant impact on outcomes research: A responsive evaluation of the international OMERACT conferences. BMJ Open, 3 (5), e002241.
[2] International Association for Public Participation. (2018). IAP2 spectrum of public participation .
[3] Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8 (1), 19–32.
[4] Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M.G., Garritty, C., … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169 (7), 467–473.
[5] Brand, A., Allen, L., Altman, M., Hlava, M., & Scott, J. (2015). Beyond authorship: Attribution, contribution, collaboration, and credit. Learned Publishing, 28 (2), 151–155.
Acknowledgments: NIL.
Disclosure of Interests: None declared.