fetching data ... 
Background: Interleukin-17A (IL17A) is a key pathogenic cytokine in spondyloarthritis (SpA) and a validated therapeutic target of secukinumab. However, circulating IL-17A levels often increase during IL-17A blockade, complicating their interpretation as biomarkers of disease activity. Conventional assays do not distinguish free cytokine from antibody-bound IL-17A, highlighting the need for improved approaches to understand IL-17A dynamics during treatment.
Objectives: To investigate the dynamics of IL-17A levels in patients with spondyloarthritis (SpA) treated with secukinumab and to determine the relationship between circulating IL-17A forms and clinical response.
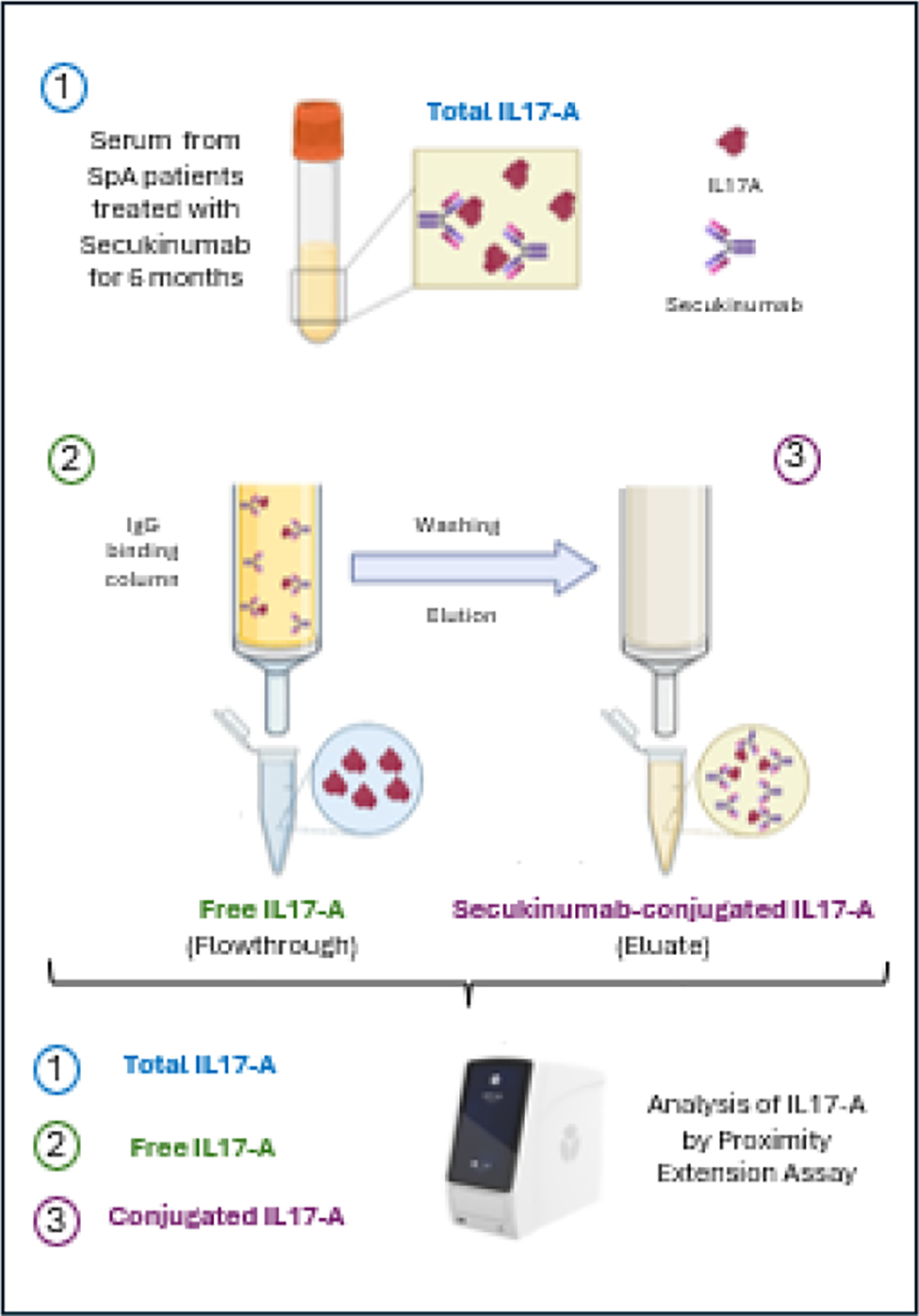
Methods: We analyzed serum IL-17A levels in 33 samples from 11 SpA patients using the highly sensitive proximity extension assay (PEA) at baseline and after 6 and 12 months of secukinumab treatment. Clinical parameters including ASDAS and CRP were recorded. To distinguish free IL- 17A from secukinumab-bound IL-17A, we developed an innovative IgG column-based assay that separates free cytokine from antibody-conjugated fractions.
Results: Serum IL-17A levels significantly increased at 6 and 12 months post-secukinumab treatment. This increase correlated negatively with ASDAS and CRP, indicating better clinical response. Analysis showed that the rise was mainly due to the secukinumab-bound IL-17A fraction, while free IL-17A levels remained stable.
Conclusions: Our study reveals that the elevated IL-17A levels detected after secukinumab treatment primarily represent the antibody-conjugated form rather than free cytokine. This conjugated fraction is associated with improved clinical outcomes, suggesting it could serve as a biomarker for therapeutic efficacy. The novel IgG column-based assay provides a valuable tool for differentiating cytokine forms in patients undergoing monoclonal antibody therapies, with potential applications beyond SpA. These findings advance understanding of IL-17A dynamics during treatment and open new avenues for personalized monitoring and management in autoimmune diseases.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.