fetching data ... 
Background: Fibromyalgia affects 2-4% of the global population, predominantly women, causing chronic widespread pain, fatigue, sleep disturbances, and functional impairment. Despite numerous available treatments, optimal management strategies remain controversial. Recent years have witnessed emergence of novel therapeutic approaches including multicomponent interventions, digital therapies, and neuromodulatory techniques. Contemporary evidence synthesis is needed to guide clinical decision-making and optimize patient outcomes.
Objectives: To systematically evaluate and compare the efficacy of pharmacological and non-pharmacological interventions for pain reduction and functional improvement in adult patients with fibromyalgia, based on randomized controlled trials published 2020-2025, with focus on effect sizes, numbers needed to treat, and clinically meaningful improvement rates.
Methods: Semantic search across 138 million papers (Elicit/Semantic Scholar). Inclusion: RCTs 2020-2025, Q2+ journals, adults with fibromyalgia (ACR criteria), interventions ≥8 weeks, pain/functional outcomes. From 500 articles, 114 met criteria; 40 highest-scoring selected. Data extracted: intervention details, outcomes (VAS, NRS, BPI, FIQ/FIQR), effect sizes (Cohen’s d), NNT, responder rates (≥30%/≥50% pain reduction)
Results: Forty RCTs analyzed (n=20-560): 33 non-pharmacological, 7 pharmacological.
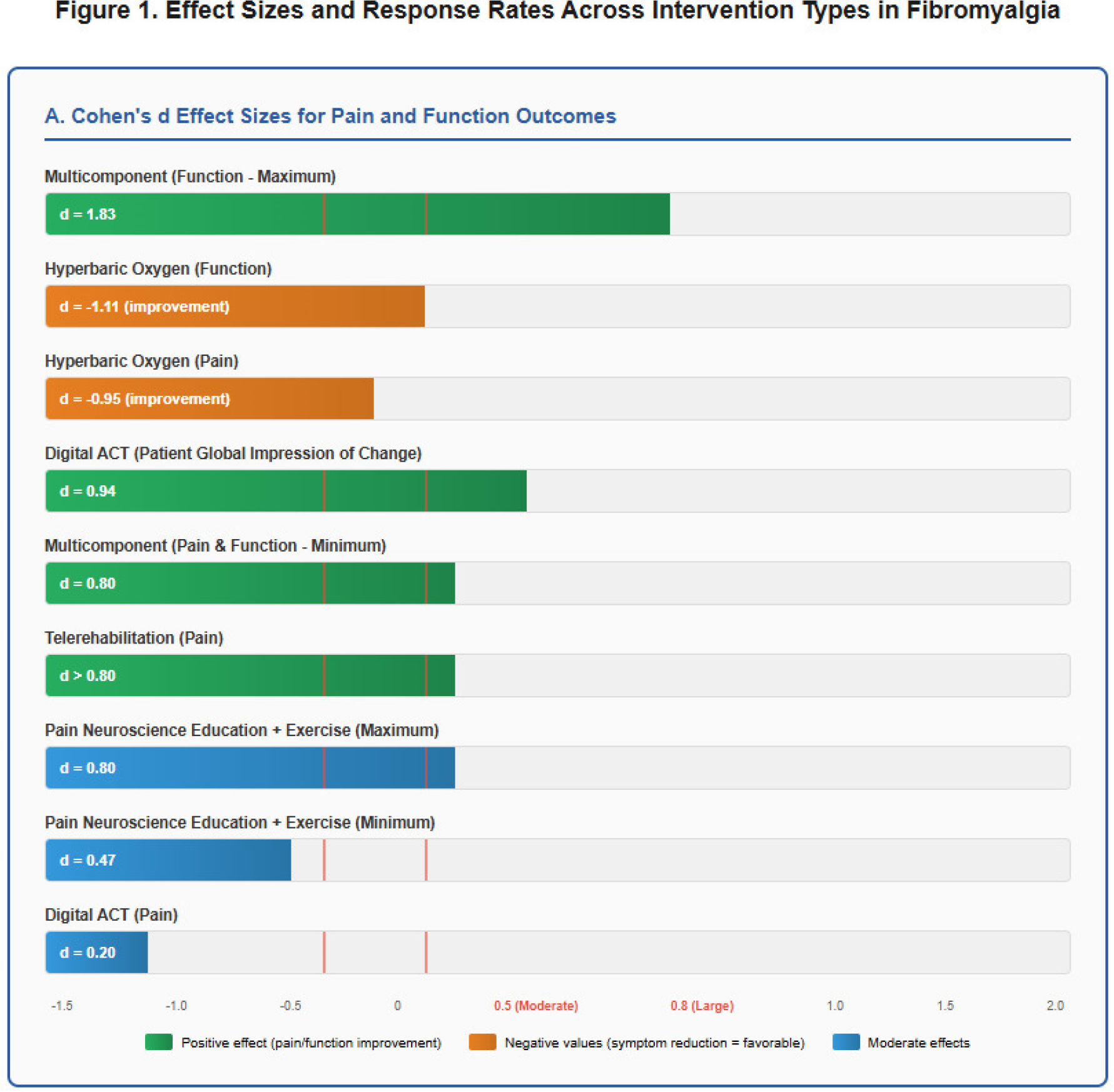
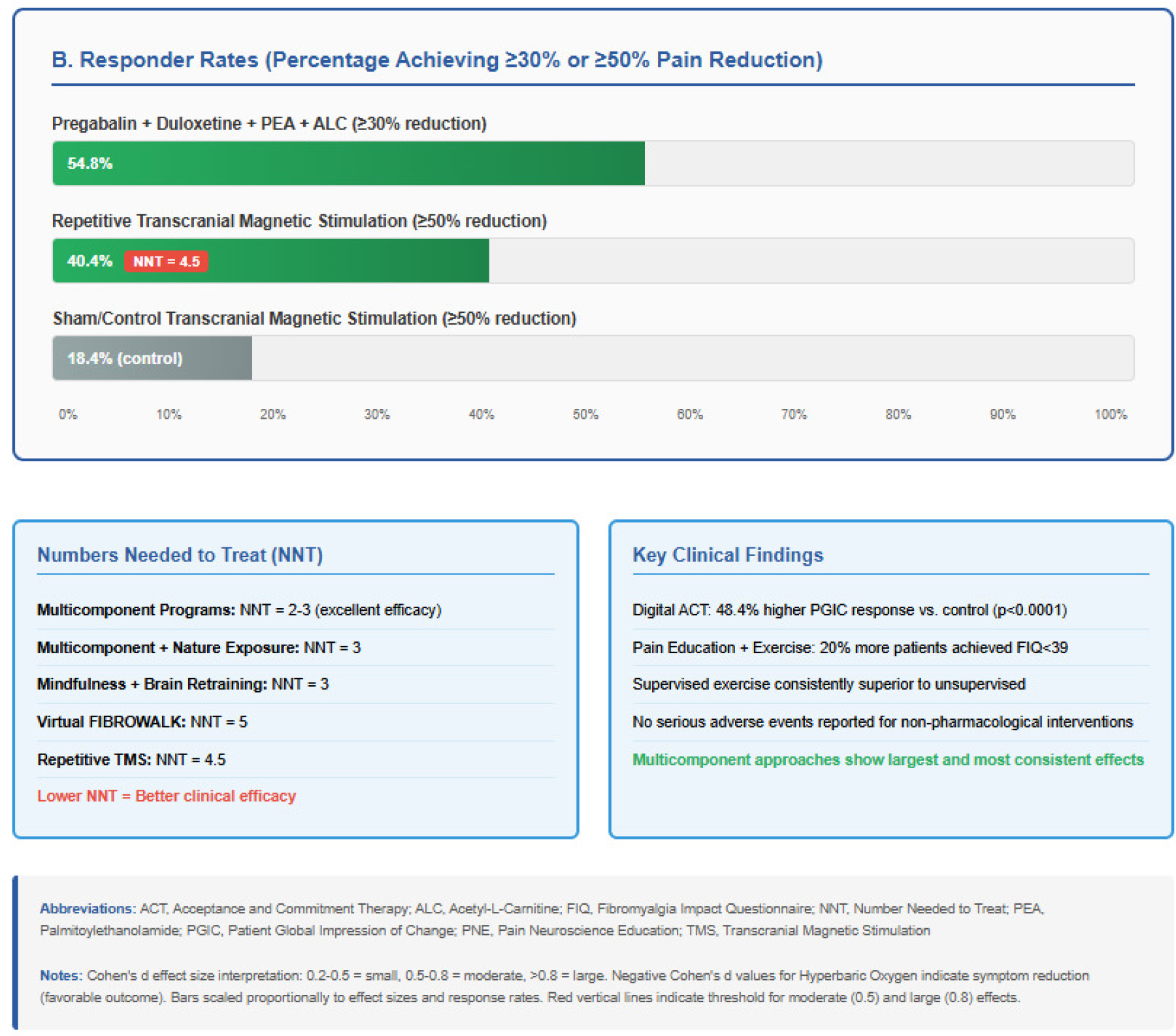
Non-pharmacological: Multicomponent programs (pain neuroscience education+exercise+CBT+mindfulness) showed largest effects: Cohen’s d>0.80 for pain and function, NNT=2-3. Multicomponent plus nature exposure achieved d=1.13-1.83 for function, NNT=3. Mindfulness plus amygdala/insula retraining: large pain effects, NNT=3.
Digital therapies: acceptance-commitment therapy achieved d=0.94 for PGIC, 48.4% higher response (p<0.0001). Virtual programs: NNT=5. Telerehabilitation: d>0.8 for pain.
Pain education plus exercise: large pain effects, 20% more patients achieving FIQ<39. Supervised exercise superior to unsupervised when combined with medications.
Pharmacological/neuromodulatory: Pregabalin+duloxetine+palmitoylethanolamide+acetyl-L-carnitine: 54.8% responders (≥30% pain reduction), significant functional improvement (p=0.033).
Repetitive transcranial magnetic stimulation: ≥50% pain reduction in 40.4% vs 18.4% sham, NNT=4.54. Hyperbaric oxygen: d=-0.95 (pain), d=-1.11 (function) vs medication.
Safety: No serious adverse events reported for non-pharmacological/digital interventions. Pharmacological interventions reported as safe.
Conclusions: Multicomponent non-pharmacological interventions combining pain neuroscience education, exercise, CBT, and mindfulness demonstrate superior efficacy with large effect sizes (d>0.80) and low NNT (2-3). Digital/telerehabilitation modalities offer accessible alternatives with comparable efficacy.
Among pharmacological approaches, pregabalin-duloxetine combinations with nutraceuticals achieved clinically meaningful benefits in >50% patients. Neuromodulatory techniques (TMS, hyperbaric oxygen) provide promising options for refractory cases with large effects.
Clinical implications support prioritizing multicomponent programs first-line, with selective incorporation of digital platforms and pharmacotherapy for inadequate responders. The superior performance of multidisciplinary approaches underscores fibromyalgia’s multifactorial nature requiring simultaneous addressing of biological, psychological, and social dimensions.
Healthcare systems should invest in structured multicomponent programs and telemedicine platforms. Future research: comparative effectiveness trials, predictive biomarkers, long-term outcomes, implementation strategies.
REFERENCES: [1] Serrat M, et al. Phys Ther. 2020;100(9):1549-65.
[2] Serrat M, et al. J Clin Med. 2020;9(10):3348.
[3] Sanabria-Mazo JP, et al. J Clin Med. 2020;9(11):3593.
[4] Catella S, et al. J Behav Med. 2023;46(4):645-57.
[5] Gendreau RM, et al. Lancet. 2024;404(10449):205-16.
[6] Serrat M, et al. Int J Environ Res Public Health. 2021;18(4):1454.
[7] Hernando-Garijo I, et al. Int J Environ Res Public Health. 2021;18(4):2075.
[8] Areso-Bóveda PB, et al. BMC Musculoskelet Disord. 2022;23(1):596.
[9] Zhang C, et al. J Med Internet Res. 2025;27:e52847.
[10] Salaffi F, et al. Clin Exp Rheumatol. 2023;41(7):1501-9.
[11] Silva VA, et al. Br J Anaesth. 2025;134(1):177-86.
[12] Ablin J, et al. PLoS One. 2023;18(10):e0288982.
Acknowledgments: NIL.
Disclosure of Interests: None declared.