fetching data ... 
Background: Axial spondyloarthritis (axSpA) is a chronic inflammatory disease historically considered to predominantly affect males. However, emerging evidence indicates an increasing prevalence among female patients, accompanied by sex-specific differences in pathophysiology and disease manifestations. Whether these differences translate into variations in medication utilization and healthcare costs in real-world practice remains unclear.
Objectives: To assess sex differences in medication utilization and axSpA-related healthcare costs.
Methods: Patients with confirmed radiographic axSpA (ICD-10 code M45; rare intractable disease code V140) diagnosed between 2020 and 2022 were identified using the Korean National Health Insurance Service database (2010–2023). Medication utilization and healthcare costs were assessed during the first year following confirmed axSpA diagnosis was assessed. AxSpA-related healthcare costs included outpatient visits, inpatient care, pharmacy-related expentirues, and were reported on a per-patient-per-year basis in US dollars. A generalized linear model with a gamma distribution and log link to examine factors associated with axSpA-related healthcare costs
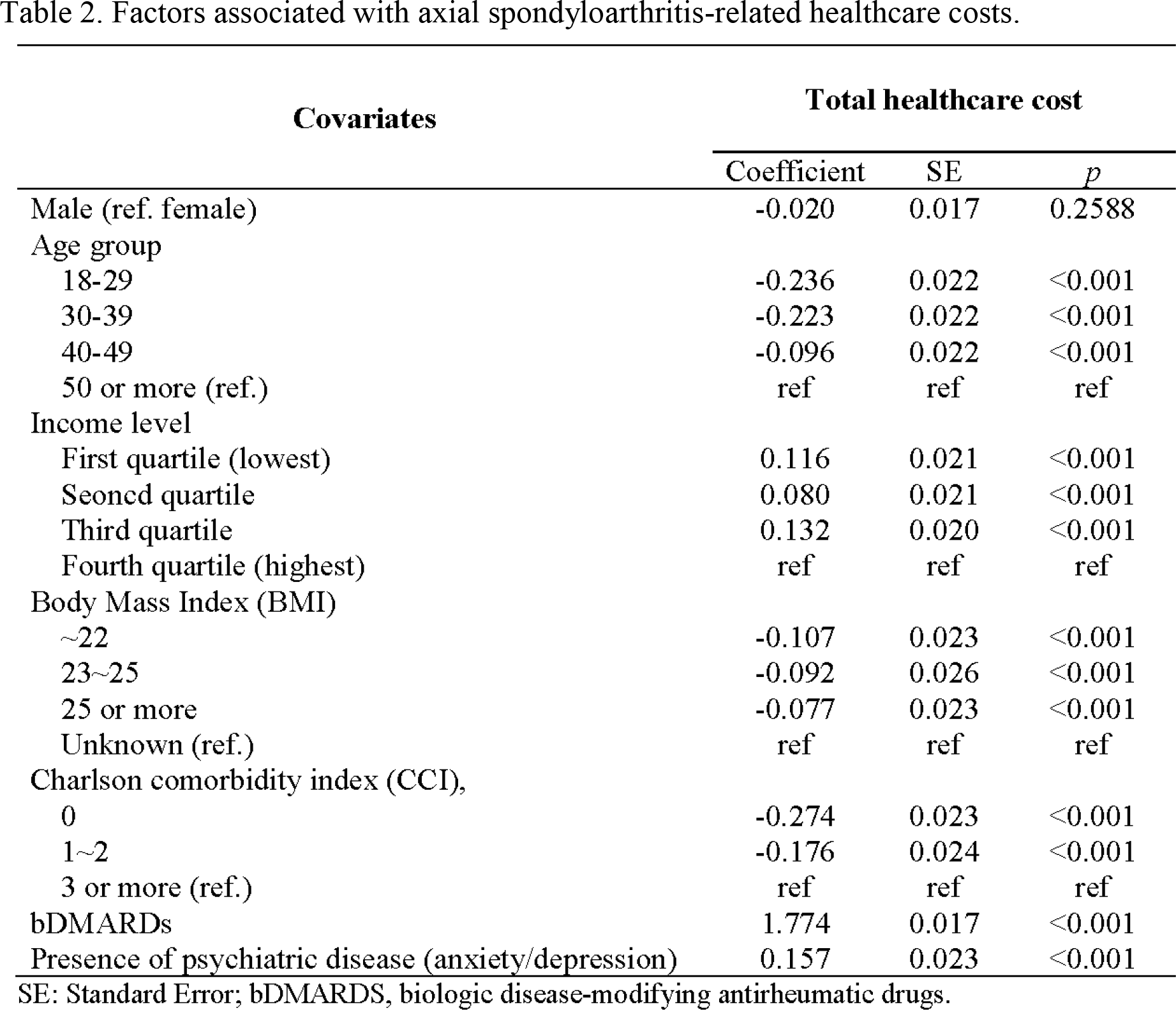
Results: Among 11,083 patients with radiographic axSpA, 7,825 were male and 3,258 were female. Female patients were diagnosed at an older age than male patients (42.8 years, Standard deviation [SD] 14.9 vs. 39.2 years, SD 15.3; p <0.001) and had higher Charlson comorbidity index scores (1.2, SD 1.4 vs 1.0, SD 1.4; p <0.001). Female patients more frequently prescribed Nonsteroidal anti-inflammatory drugs (NSAIDs), conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), corticosteroids, and analgesics, whereas biologic disease-modifying antirheumatic drugs (bDMARDs) were more commonly prescribed among male patients (28.1% vs. 25.9%, p =0.02). AxSpA-specific healthcare costs were higher among male patients (1,984.42 USD vs. 1,945.41 USD), while female patients incurred slightly higher inpatient costs. In cost regression analyses, sex was not statistically significant covariates of total costs; instead, bDMARD use was highly associated with the axSpA-related healthcare cost (β=1.774, p <0.001).
Conclusions: In real-world practice, sex differences were observed in medication utilization, particularly in bDMARD use, and axSpA–related healthcare costs were primarily driven by bDMARD use rather than sex.
Table 1. Medication utilization and axial spondyloarthritis-related healthcare costs by sex.
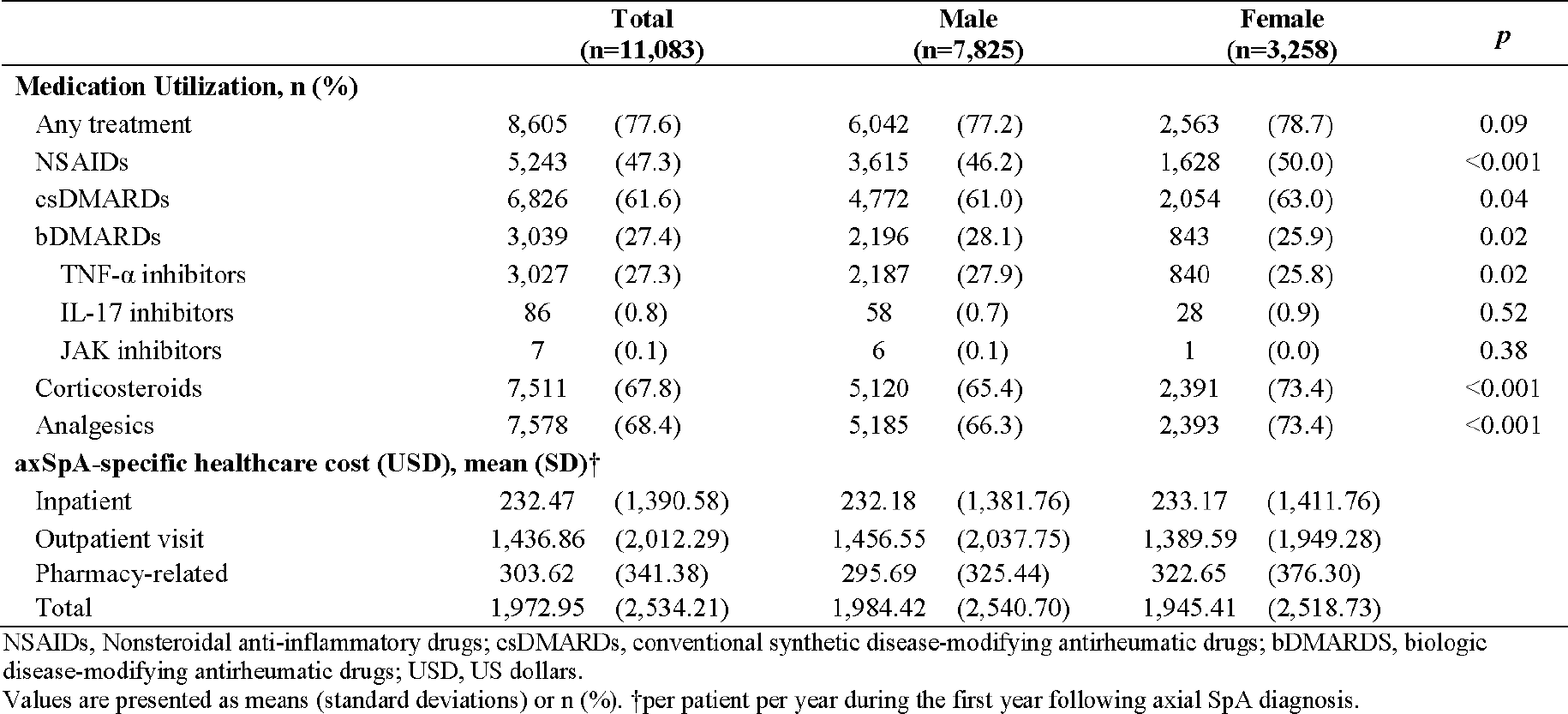
Table 2. Factors associated with axial spondyloarthritis-related healthcare costs.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.