fetching data ... 
Background: Avacopan is an oral C5a receptor (C5aR) antagonist that inhibits the alternative complement pathway and neutrophil activation, key mechanisms in the pathogenesis of ANCA-associated vasculitis (AAV). The phase 3 ADVOCATE trial demonstrated non-inferiority of avacopan compared with a standard prednisolone taper for remission at 26 weeks and superiority for sustained remission at 52 weeks, with improved renal recovery [1,2]. However, patients with severe renal impairment (estimated glomerular filtration rate [eGFR] <15 mL/min) were excluded, follow-up was limited to one year, and induction therapy was restricted to rituximab or cyclophosphamide alone. Combination induction therapy, commonly used in severe renal or pulmonary disease, and routine maintenance immunosuppression after rituximab were not evaluated.
Objectives: To assess the real-world efficacy, safety, and glucocorticoid-sparing effects of avacopan in patients with severe AAV, including those receiving combination induction therapy.
Methods: We conducted a retrospective single-centre study including patients with new-onset or relapsing granulomatosis with polyangiitis (GPA) or microscopic polyangiitis (MPA), diagnosed according to the 2022 ACR/EULAR criteria, with organ- or life-threatening disease. Patients treated with avacopan in combination with standard remission induction therapy (rituximab, cyclophosphamide, or both) were compared with matched controls receiving standard therapy without avacopan. Matching (1:2) was performed using a manual nearest-neighbour approach based on age, sex, disease status (new-onset vs relapse), Birmingham Vasculitis Activity Score (BVAS), disease subtype, organ involvement, induction regimen, and comorbidities. The primary endpoints were remission (BVAS=0 and prednisolone ≤5 mg/day) at 6 and 12 months. Secondary endpoints included relapse, time to remission, cumulative glucocorticoid exposure, renal function, adverse events, and avacopan discontinuation
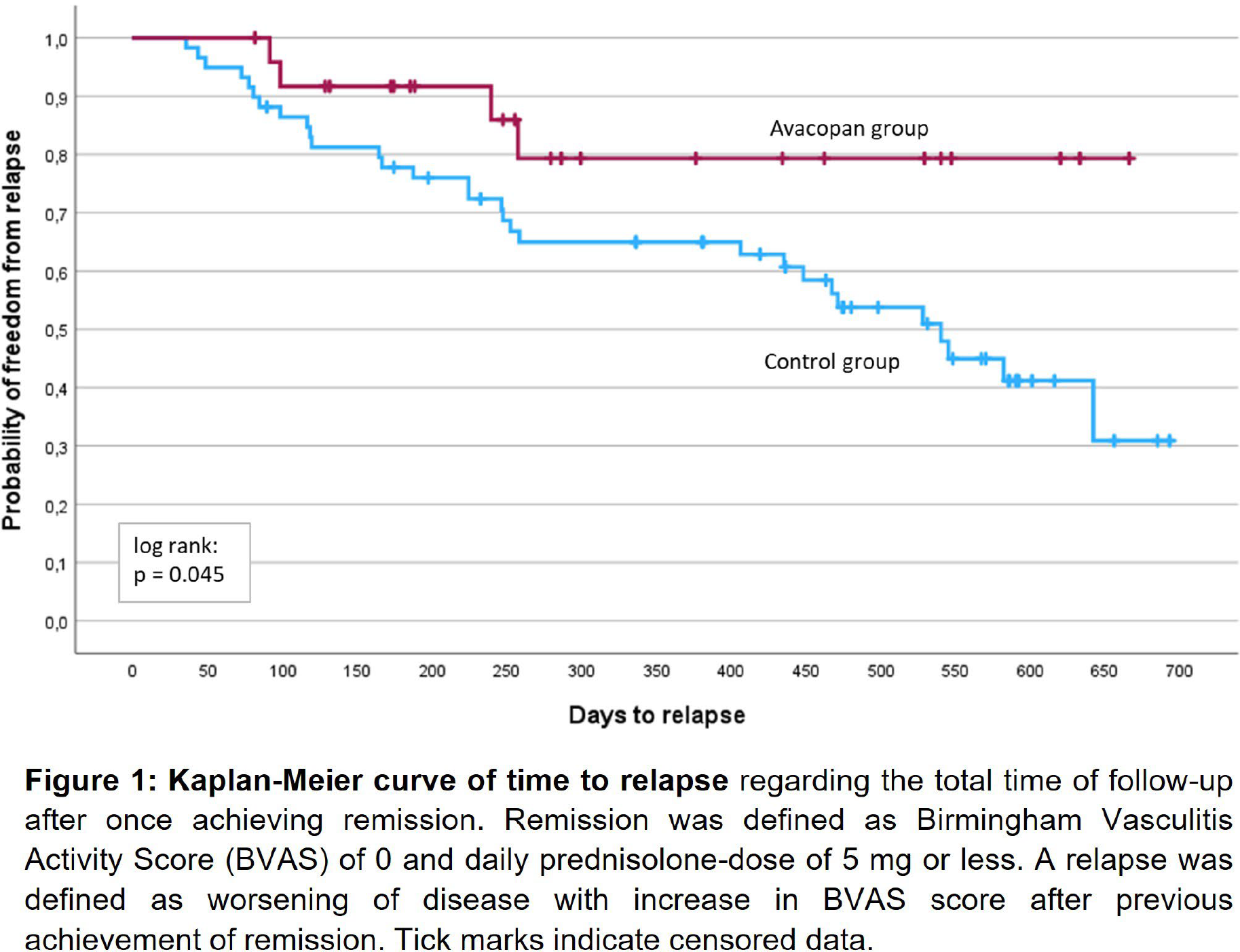
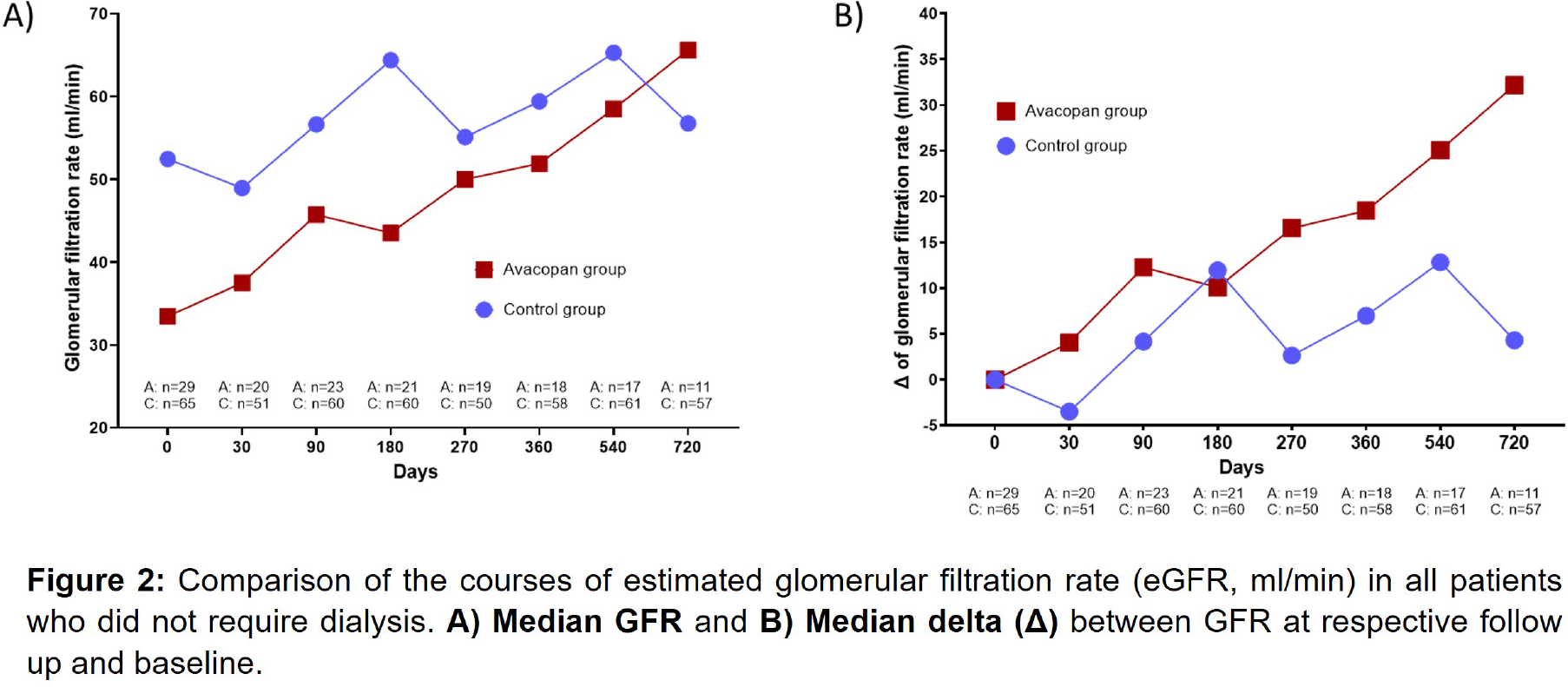
Results: Thirty-five patients treated with avacopan were compared with 70 matched controls. Median age was 62 years, 55% had GPA, and 79% had new-onset disease. Median baseline BVAS was 15 (IQR 12–20). Baseline characteristics were comparable, although median eGFR was lower in the avacopan group (24 vs 49 mL/min). Induction therapy reflected severe disease and included rituximab (28%), cyclophosphamide (10%), or combined rituximab and cyclophosphamide (62%). Remission rates were similar at 6 months (69% vs 68%) but higher with avacopan at 12 months (86% vs 68%; p=0.11). Median time to remission did not differ significantly (169 vs 195 days; p=0.30). During follow-up, relapses occurred less frequently in the avacopan group (16% vs 51%; p=0.003), including after treatment cessation. Kaplan–Meier analysis demonstrated a significantly lower cumulative relapse risk with avacopan (log-rank p=0.045). Avacopan was associated with accelerated glucocorticoid tapering (≤5mg/day; 102 vs 164 days, p<0.001), with lower cumulative glucocorticoid doses (3266 vs 4288 mg; p=0.008). Renal recovery was greater with avacopan (ΔeGFR +18 vs +7 mL/min at 12 months), and median eGFR exceeded that of controls after 24 months despite lower baseline values. Notably, 31% of avacopan-treated patients had baseline eGFR <15 mL/min, a population excluded from the ADVOCATE trial. Overall safety was comparable in both groups. Lymphopenia was more frequent in controls, while severe infections and elevated liver enzymes occurred slightly more often with avacopan, particularly within the first six weeks. Avacopan was discontinued in nine patients (26%), mainly due to lymphopenia or hepatotoxicity.
Conclusions: In real-world clinical practice, avacopan was effective and generally well tolerated in patients with severe AAV. It enabled significant glucocorticoid sparing, improved renal recovery, and reduced relapse rates, including in patients receiving combination induction therapy with rituximab and cyclophosphamide. Clinical benefits persisted beyond 12 months, supporting and extending findings from randomised clinical trials.
REFERENCES: [1] Jayne DRW, Merkel PA, Schall TJ, Bekker P. Avacopan for the Treatment of ANCA-Associated Vasculitis. N Engl J Med, 2021;384:599–609.
[2] Cortazar FB, Niles JL, Jayne DRW, Merkel PA, Bruchfeld A, Yue H, et al. Renal Recovery for Patients with ANCA-Associated Vasculitis and Low eGFR in the ADVOCATE Trial of Avacopan. Kidney International Reports, 2023;8:860–70.
Acknowledgments: NIL.
Disclosure of Interests: Franz Thiele AbbVie, Janssen, GSK, Johanna Schneider GSK, Chiesi, Eric Prager GSK, Ilona Jandova: None declared, Björn Christian Frye Advita Lifescience GmbH, Actelion, AstraZeneca, Boehringer Ingelheim, Novartis, Roche and Vifor, Advita Lifescience GmbH, Actelion, AstraZeneca, Boehringer Ingelheim, Novartis, Roche and Vifor, Bristol-Myer Squibb and Relief Therapeutics, Reinhard Voll AbbVie, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, CSL Vifor, GSK, Janssen, Novartis, Pfizer., AbbVie, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, CSL Vifor, GSK, Janssen, Novartis, Pfizer., Markus Schramm Boehringer, Novartis, AstraZeneca, Nils Venhoff UCB, Janssen, Novartis, AbbVie, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, CSL Vifor, GSK, Novartis, Pfizer, Sanofi, Janssen, AbbVie, AstraZeneca, Bristol Myers Squibb, Chugai, CSL Vifor, GSK, Novartis, Pfizer, Sanofi, Janssen, AbbVie, Novartis, Pfizer.