fetching data ... 
Background: Rheumatoid arthritis (RA) is a chronic autoimmune disease, characterized by persistent inflammation that primarily affects synovial joints, leading to progressive articular destruction, deformity, and functional impairment. Early diagnosis is critical to prevent irreversible damage, yet it remains a clinical challenge due to the heterogeneity and clinical overlap with other inflammatory arthritides. In recent years, Artificial Intelligence (AI), including machine learning (ML) and deep learning (DL), has been increasingly explored as a research approach to support RA diagnosis by integrating large, multidimensional datasets (e.g., omics, laboratory biomarkers, imaging, and clinical records). In research, AI models have repeatedly shown high diagnostic performance, often outperforming traditional statistical and threshold-based approaches.
Objectives: This scoping review aimed to map and synthesize the current evidence on AI-based approaches for RA diagnosis and closely related diagnostic tasks (such as early recognition and phenotyping). Specifically, we sought to (i) identify the main AI approaches and data sources used (ii) highlight knowledge gaps and emerging trends to inform future research and clinical translation
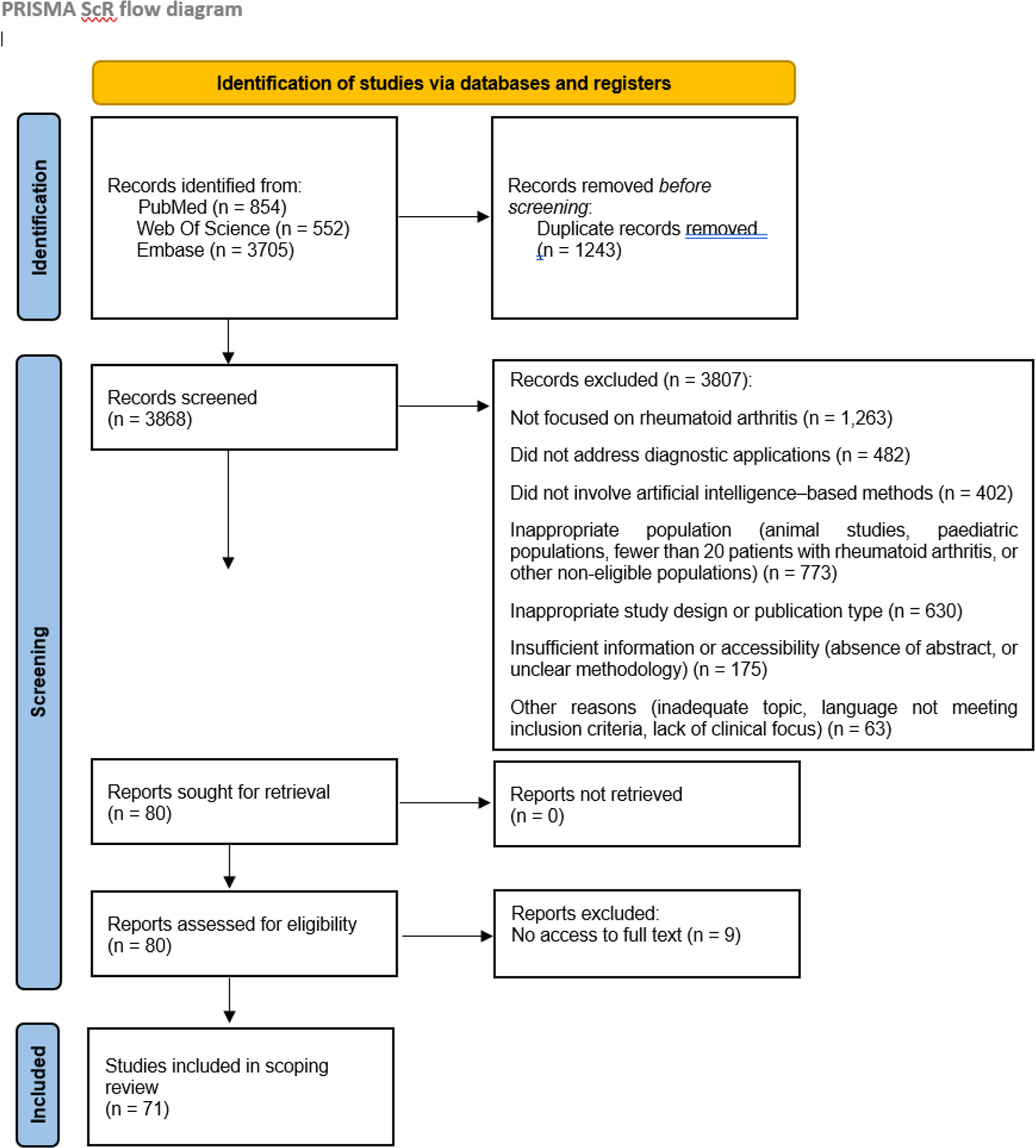
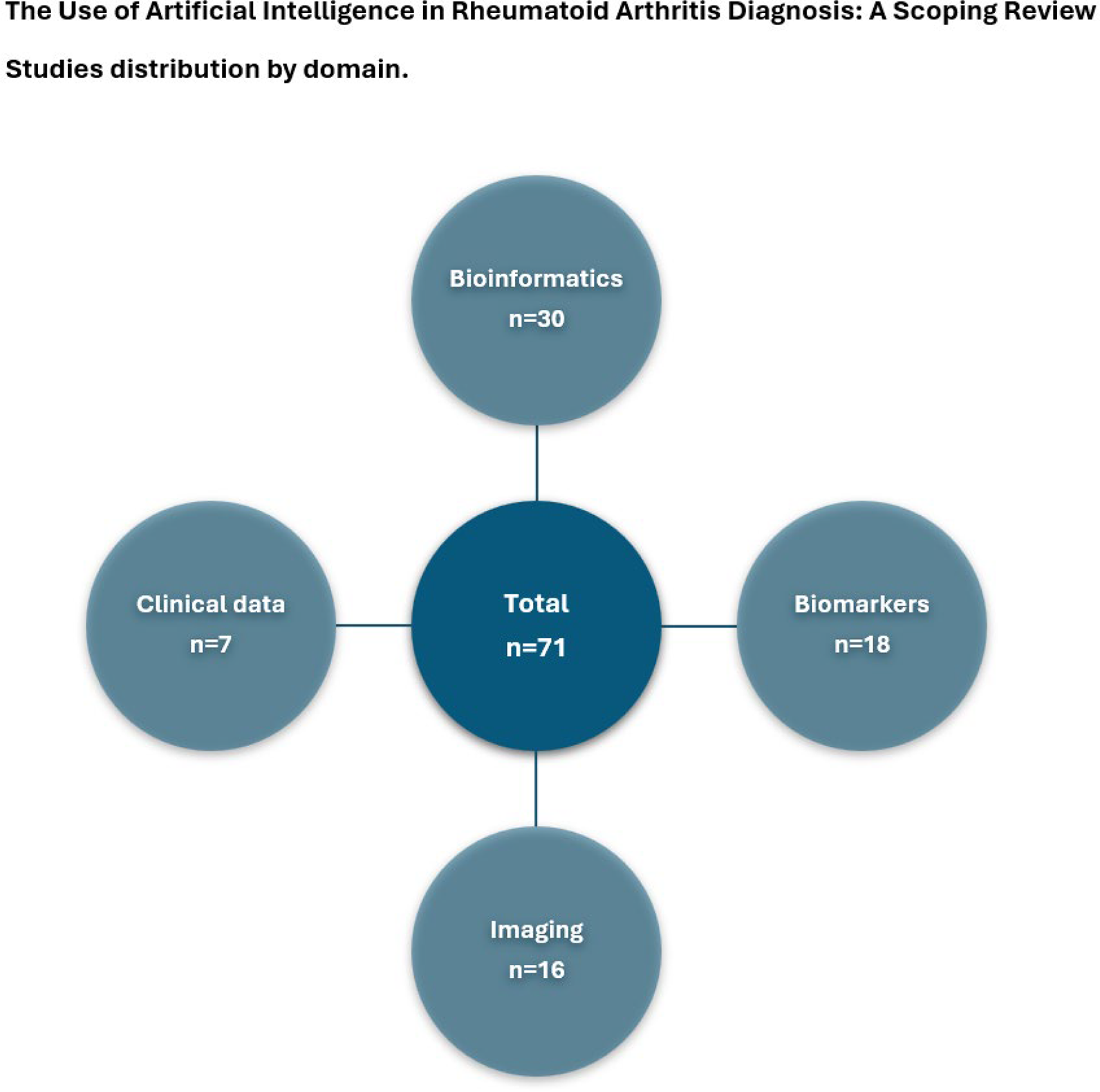
Methods: This scoping review followed PRISMA-ScR guidelines and encompassed a comprehensive and structured bibliographic search conducted in PubMed, Web of Science and Embase. In total, 5,111 records were initially identified and after removing duplicates and screening of titles/abstracts using predefined eligibility criteria full texts were assessed and 71 studies were included. Extracted data were charted and organized by primary data source modality: omics/bioinformatics, laboratory biomarkers, imaging, and clinical/electronic health record (EHR) data, to enable comparative synthesis.
Results: AI applications varied by modality and study design. In omics-focused studies, ML-based feature selection and clustering approaches identified candidate diagnostic genes, including SPP1 , FOXO3 and MMP13 . Reported discrimination was frequently high, with AUC values commonly in the 0.85–0.96 range. Deep neural networks applied to transcriptomic and single-cell datasets revealed molecular subtypes of RA as well as early patterns of immune dysregulation.
In biomarker-based studies, Random Forest and support vector machine (SVM) classifiers using serum or urinary proteomics, DNA methylation, and metabolomic profiles demonstrated excellent diagnostic discrimination, with several models (e.g., based on AIM2 and HTR2A methylation or antigenomic signatures) reporting AUCs exceeding 0.95. Artificial neural networks and boosting decision trees further enhanced sensitivity, enabling clinically meaningful classification (seropositive and seronegative RA).
In imaging studies, convolutional neural networks (CNNs) applied to radiography, MRI, ultrasound, thermography, and optical imaging commonly achieved high accuracy for RA identification and severity-related assessment (often 90–98% in internal evaluations). Notably, deep CNNs identified early inflammatory changes on MRI and thermography before they became apparent on conventional imaging, highlighting their potential for early disease recognition.
Finally, with regard to Clinical Data, machine learning algorithms leveraging electronic health records and laboratory data demonstrated robust performance in patient identification and classification. Random Forest, logistic regression and neural network models achieved accuracies ranging from 90% to 97%, with some outperforming expert-defined algorithms. The incorporation of composite laboratory variables (e.g., RF, anti-CCP and 14-3-3η) and patient medical history significantly improved predictive performance.
Conclusions: AI applications demonstrate substantial potential to improve diagnostic accuracy, as well as the timely and early diagnosis of RA across different data modalities. The integration of multi-omic, imaging, and clinical information enables effective recognition of disease-specific patterns, often beyond human interpretability. Key advantages include scalability, reproducibility, and the capacity for continuous learning. However, these models also encompass several limitations. Across domains, performance metrics and validation strategies were heterogeneous (AUC vs accuracy; internal vs external validation), limiting direct comparability. The evidence base is constrained by small and single-centre datasets, limited external validation, data heterogeneity, and variable clinical interpretability and reporting. Future research should prioritize multicentre and external validation, prospective/longitudinal designs, harmonized outcome definitions, and standardized reporting to facilitate safe translation of AI-assisted diagnostic tools into routine rheumatology practice.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.