fetching data ... 
Background: autoimmune phenomena and immune dysregulation contribute to cardiovascular risk excess in rheumatoid arthritis (RA), although exact players are ill-defined. G-coupled protein receptors (GPCR) are involved in a wide range of biological processes, such as immune response, cell traffiking and migration or neuroendocrine physiology. Autoantibodies against GPCR, such as anti-CXCR3 antibodies, have recently emerged as functional players of GPCR signaling, and being termed as regulatory antibodies. Altered levels of these antibodies may be associated with loss of tissue homeostasis. However, little evidence is available on their role in rheumatic and musculoskeletal diseases, mostly coming from studies on Sjögren disease or systemic sclerosis, whereas their role in RA remains largely unexplored.
Objectives: to evaluate anti-CXCR3 antibody levels, as well as their potential associations with disease features, atherosclerosis burden, and functional pathways, accross the whole RA spectrum.
Methods: 82 early, treatment-naïve RA patients (2010 EULAR/ACR classification criteria; 69% RF, 66% ACPA; DAS28 5.28±1.13), 14 individuals with clinical-suspect arthralgia (CSA) (54% RF, 45% ACPA) and 70 healthy controls (HC) were recruited. A validation cohort consisting of 90 established RA patients (55% RF, 63% ACPA; DAS28 3.58±1.37; median disease duration: 5.66 (range 0.50-22.83) years; CV events: n=16) and 37 HC was included. A group of 13 biological DMARD-naïve RA patients were prospectively followed for 3 months upon TNF blockade initiation. Clinical outcomes upon DMARDs followed EULAR clinical response definitions. Anti-CXCR3 antibodies were measured by commercial immunoassays (CellTrend, Germany). Atherosclerosis occurrence was measured by Doppler-ultrasound. Serum proteins were evaluated through high-throughput targeted proteomics (Olink, Sweden). Publicly available datasets (GEO NCBI) were explored to evaluate CXCR3 expression in RA studies
Results: IgG anti-CXCR3 antibodies were decreased in early RA patients (p<0.010) and CSA individuals (p=0.045) compared to HC. Equivalent results were obtained in the validation cohort (p<0.001). Anti-CXCR3 antibodies were unrelated to clinical features, including disease activity (DAS28: r=-0.061, p=0.589; CDAI: r=-0.057, p=0.612), joint counts (tender: r=-0.044, p=0.697; swollen: r=-0.044, p=0.694), HAQ (r=-0.195, p=0.083), symptom duration (r=-0.003, p=0.980), or disease-related autoantibodies (RF, p=0.948; ACPA: p=0.999). A negative association was found with ANA positivity (p=0.037). Lower anti-CXCR3 antibodies at baseline were associated with poor therapeutic responses at 6 (p=0.002) and 12 months (p=0.020) in early RA patients upon csDMARD initiation. However, anti-CXCR3 antibodies were unchanged upon TNF blockade (p=0.560), regardless of treatment outcomes (responders: p=0.625, moderate/non-responders: p=0.945).
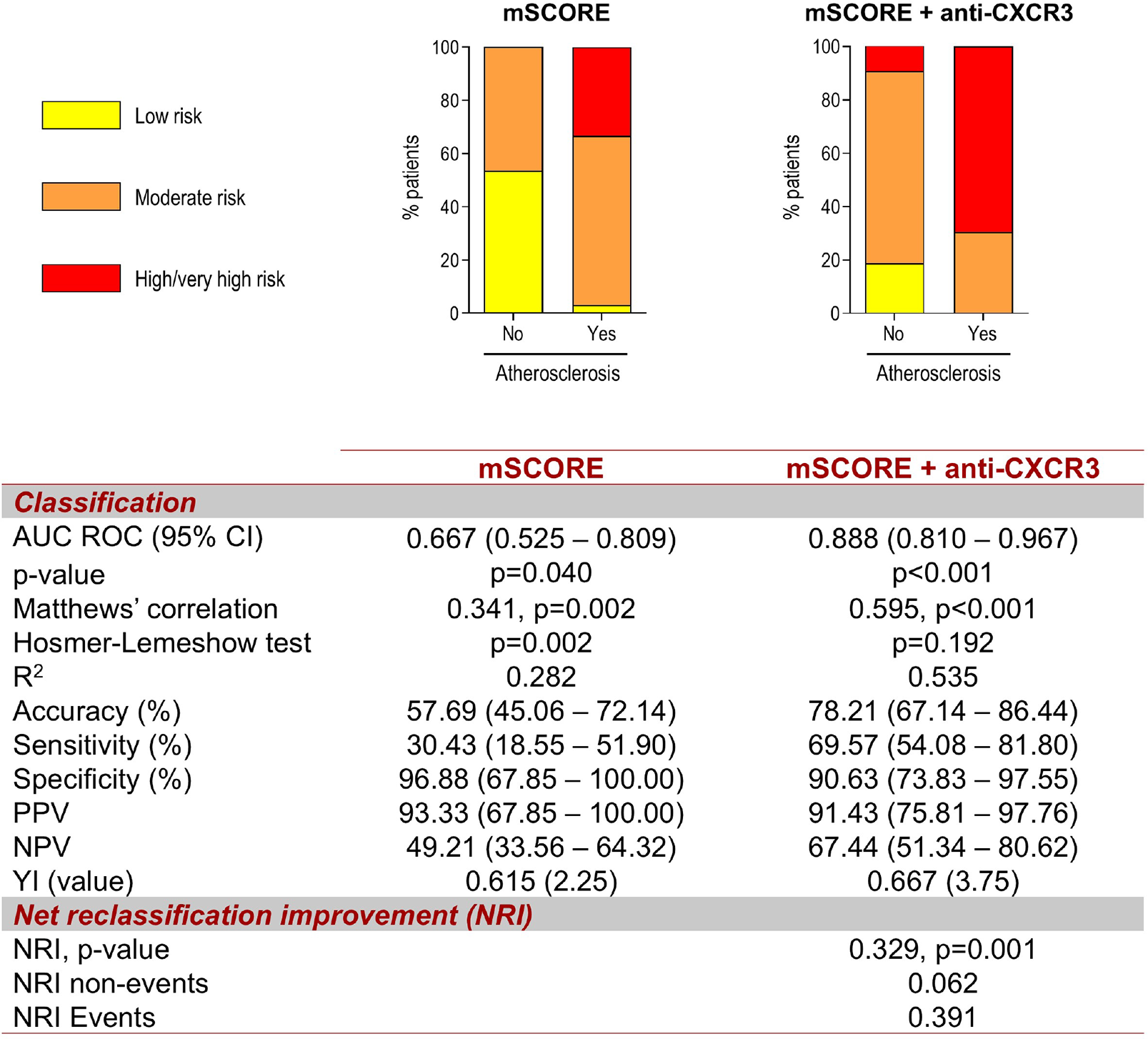
Anti-CXCR3 antibodies did not exhibit associations with traditional CV risk factors (dyslipidemia, hypertension, diabetes, smoking and diabetes) (all p>0.050). Lower anti-CXCR3 levels were associated with atherosclerosis occurrence (p=0.010) and extent (r=-0.248, p=0.020) in early RA patients. Anti-CXCR3 levels were associated with of atherosclerosis occurrence in early RA in univariate models (OR [95% CI]: 0.967 [0.942-0.993], p=0.012) and remained as independent predictors in multivariate models adjusted for traditional risk factors (0.939 [0.890-0.990], p=0.019). This association was confirmed in the validation cohort (p=0.045). Moreover, adding anti-CXCR3 levels to the mSCORE improved risk stratification over the mSCORE alone based on diagnostic and classification statistics and net reclassification improvement (Figure 1).
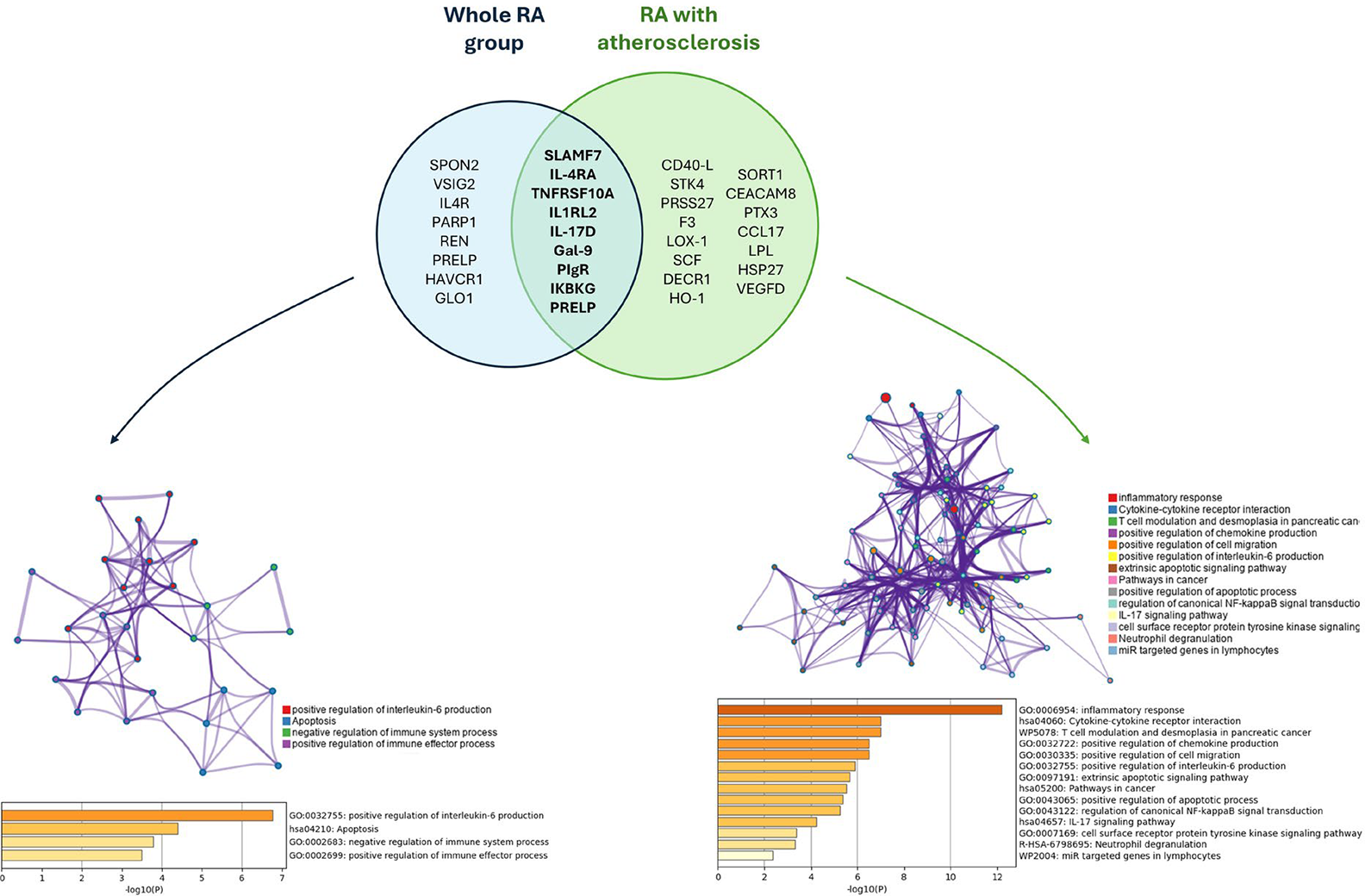
Proteomic analyses revealed that anti-CXCR3 antibodies were associated with 15 proteins (protein-protein interaction enrichment: p<0.005) in early RA related to broad immune activation and inflammatory pathways (Figure 2). Subgroup analyses in patients with atherosclerosis revealed a richer protein network (24 protein hits, PPI enrichment: p=1.25·10 -5 ), which included a number of proteins functionally connected with cardiovascular disease (F3, LOX-1, HO-1, SPRT1, CEACAM, PTX3, LPL, and HSP27), and informed pathways related to specific immune circuits, apoptosis, and chemotaxis (Figure 2B).
The analysis of public datasets revealed a consistent increase in CXCR3 expression in synovial tissue across gene sets (GSE1919, GSE55457, GSE55584, GSE55235, GSE36700; all p(FDR)<0.050); whereas a decreased expression was registered in blood (GSE15573 and GSE17755; p(FDR)<0.050) in RA studies.
Conclusions: altered anti-CXCR3 antibody levels may be a common hallmark along the whole RA spectrum, being found already at the earliest stages. Local accumulation/consumption due to altered trafficiking may underie these findings. Decreased anti-CXCR3 antibodies were associated with poor therapeutic outcomes, atherosclerosis burden, and functional proteomic pathways. Anti-CXCR3 antibodies hold promise as biomarkers for risk stratification. These findings demonstrate for the first time altered levels of anti-GPCR antibodies in RA. Regulatory autoantibodies may be essential in shaping our understanding of functional antibodies in human disease.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.