fetching data ... 
Background: Osteoarthritis (OA) is increasingly recognized as a heterogeneous joint disease in which synovial inflammation plays a relevant pathogenic role. Histological synovitis is frequently observed in advanced OA and has been associated with pain, structural damage, and systemic inflammatory markers. Standardized synovitis grading and the identification of synovial inflammatory pathotypes have revealed distinct immune architectures in inflammatory arthritis and, more recently, in OA. However, data integrating synovial pathotypes with clinical, laboratory, and radiographic features in large surgical OA cohorts remain limited.
Objectives: To comprehensively characterize the severity of synovial inflammation and the distribution of synovial inflammatory pathotypes in patients with advanced OA undergoing orthopedic surgery, and to investigate their associations with demographic, clinical, laboratory, and radiographic features across different joint sites
Methods: Synovial tissue samples were collected intraoperatively from adult patients undergoing primary orthopedic surgery for clinically and radiographically confirmed OA at a tertiary referral center. Procedures involved predominantly large weight-bearing joints (knee and hip), with additional samples obtained from other synovial joints. Hematoxylin and eosin–stained sections were evaluated using the standardized Krenn synovitis score, which integrates lining-layer hyperplasia, stromal cellularity, and inflammatory infiltrates, and classified as no synovitis (0–1), low-grade (2–4), or high-grade (≥5).
Immunohistochemical staining for CD3 (T cells), CD20 (B cells), CD68 (macrophages), and CD138 (plasma cells) was performed and semi-quantitatively scored to define synovial inflammatory pathotypes as lympho-myeloid, diffuse-myeloid, or pauci-immune according to established criteria.
Demographic data, body mass index (BMI), preoperative pain intensity, laboratory parameters (including hemoglobin and C-reactive protein), and derived systemic inflammatory indices—neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII)—were retrieved from medical records. Radiographic severity was assessed using the Kellgren–Lawrence grading system. Continuous variables were compared using Kruskal–Wallis tests with Dunn post-hoc correction, and categorical variables using Fisher’s exact test.
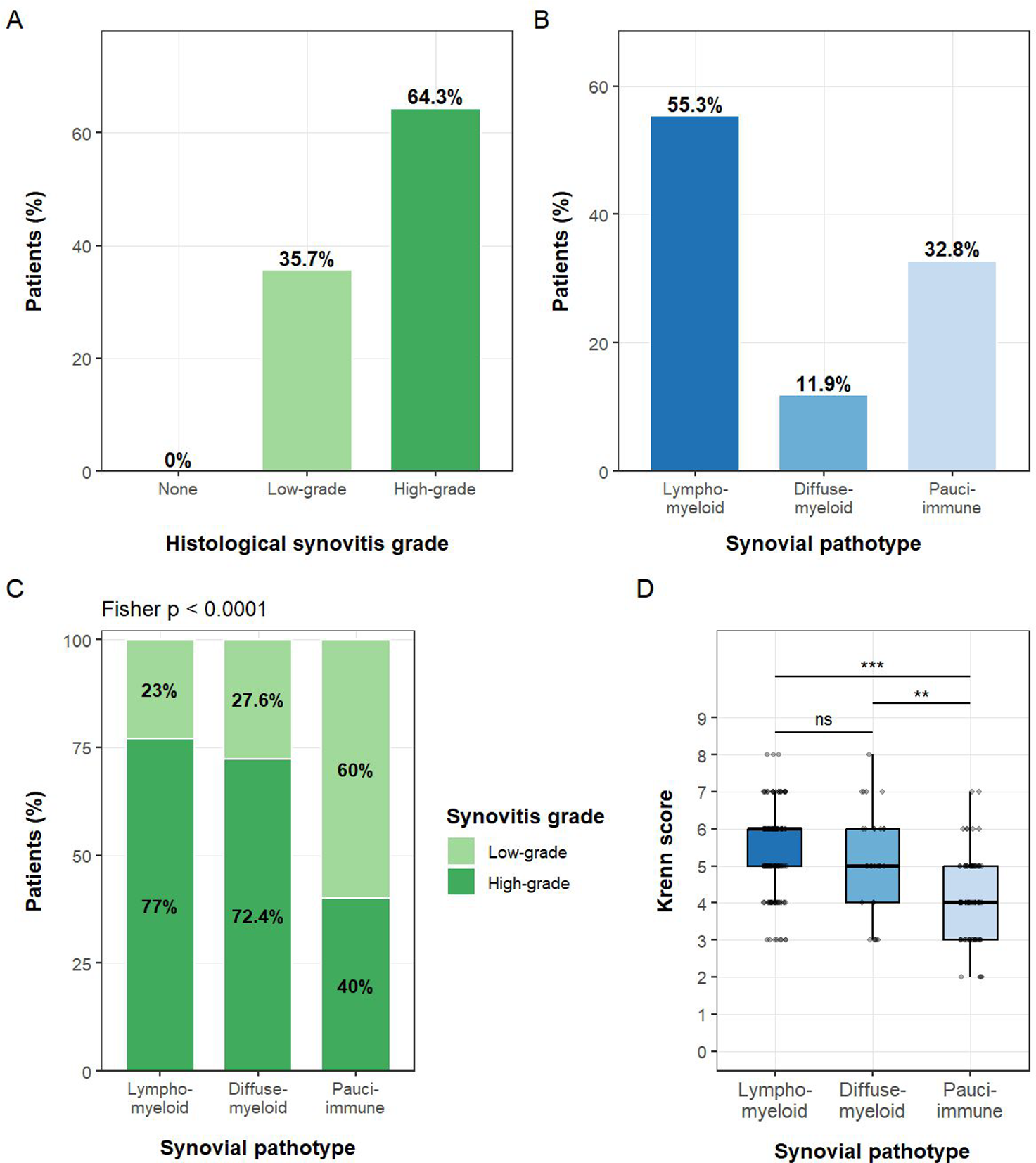
Results: A total of 244 synovial specimens were analyzed. The overall median Krenn score was 5 (IQR 4–6), indicating a substantial inflammatory burden, with 64.3% of samples classified as high-grade synovitis and 35.7% as low-grade; no specimen showed absent synovitis (Figure 1A).
The lympho-myeloid pathotype was the most prevalent inflammatory pattern (55.3%), followed by pauci-immune (32.8%) and diffuse-myeloid (11.9%) pathotypes (Figure 1B). Although all three pathotypes encompassed both low- and high-grade synovitis, their distribution differed markedly. High-grade synovitis was present in 77.0% of lympho-myeloid samples, 72.4% of diffuse-myeloid samples, and only 40.0% of pauci-immune samples (Figure 1C; Fisher p<0.0001).
A clear histological inflammatory gradient emerged across pathotypes. Median total Krenn scores increased progressively from pauci-immune [4 (IQR 3–5)] to diffuse-myeloid [5 (IQR 4–6)] and lympho-myeloid tissues [6 (IQR 5–6)] (Kruskal–Wallis p<0.001). Post-hoc analyses confirmed significantly higher scores in lympho-myeloid and diffuse-myeloid synovium compared with pauci-immune tissue (p<0.001 and p=0.001, respectively), with no significant difference between the two myeloid-rich groups (Figure 1D).
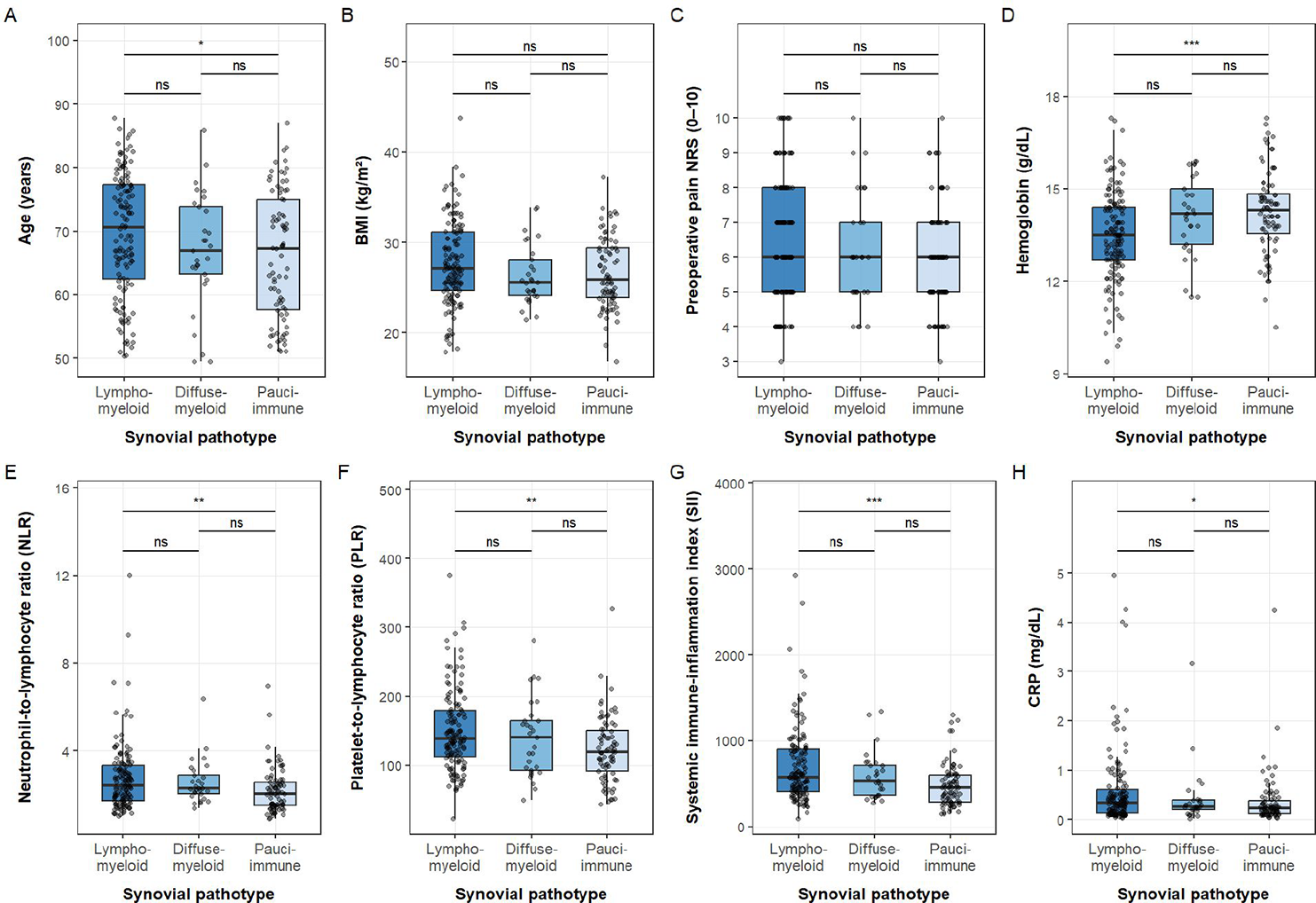
Across clinical and laboratory parameters (Figure 2A–H), age differed modestly between pathotypes (p=0.038), whereas BMI (p=0.120) and preoperative pain intensity (p=0.059) were comparable. Hemoglobin levels differed significantly (p<0.001), with lower values observed in the lympho-myeloid group compared with pauci-immune synovium (p<0.001). Systemic inflammatory indices demonstrated a consistent stepwise increase from pauci-immune to lympho-myeloid pathotypes. NLR (p=0.003), PLR (p=0.003), SII (p<0.001), and CRP (p=0.033) were all significantly higher in lympho-myeloid compared with pauci-immune samples, while no significant differences were observed between lympho-myeloid and diffuse-myeloid tissues.
In multivariable logistic regression adjusting for age, sex, BMI, systemic inflammatory indices, hemoglobin, pain intensity and duration, radiographic severity, comorbidity burden, and joint site, higher BMI emerged as the only independent predictor of the lympho-myeloid pathotype (OR 1.11, 95% CI 1.01–1.22; p=0.028), whereas Kellgren–Lawrence grade, CRP, and preoperative pain did not retain independent associations.
When stratified by anatomical site, the prevalence of high-grade synovitis was comparable across joints (63.5% knee, 65.6% hip, 68.8% other joints; p=0.924), indicating a consistent inflammatory burden irrespective of location. However, synovial pathotype distribution differed significantly by joint site (p=0.025): lympho-myeloid synovium predominated in hip and knee samples, whereas pauci-immune patterns were relatively more frequent in smaller joints. Joint site was not an independent determinant of lympho-myeloid infiltration in multivariable analysis.
Conclusions: Advanced OA synovium obtained at the time of surgery displays a high prevalence of active inflammation and reproducible immune inflammatory pathotypes. Synovial pathotypes capture a robust histological and systemic inflammatory gradient, ranging from pauci-immune to lympho-/diffuse-myeloid profiles, that is not explained by pain severity or radiographic stage alone. These findings reinforce the concept of OA as a heterogeneous inflammatory disease and support the relevance of tissue-based immune stratification to refine disease characterization and guide future mechanistic and translational research.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.