fetching data ... 
Background: Despite one of the strongest known HLA-disease associations, most HLA-B27 carriers never develop axial spondyloarthritis (axSpA), implying that additional environmental factors are required for disease initiation. One explanation is that HLA-B27 presents microbial peptides that elicit cross-reactive autoreactive T-cell responses (the arthritogenic peptide hypothesis). Recent human studies provide direct mechanistic support, showing that disease-associated T-cell receptors from axSpA patients can recognise microbial peptides presented by HLA-B27 [1]. The gut is a plausible source of relevant microbial triggers, supported associations between axSpA risk loci and gut microbiome composition (e.g., FUT2 and ABO [2]). Although observational studies have linked infections to subsequent axSpA risk, most have not defined exposure timing relative to disease onset and have not examined whether antimicrobial treatment—an established and potentially modifiable disruptor of the gut microbiome—may contribute to risk.
Objectives: To examine the association between long-term or recurrent antibiotic use during childhood and later axSpA among HLA-B27-positive individuals.
Methods: We conducted an observational analysis in UK Biobank. Participants were included if they completed the childhood antibiotic questionnaire item, were HLA-B27:05 positive (by imputation), and were of White European ancestry (to maximise HLA imputation accuracy). Classical four-digit HLA alleles were imputed using HLA*IMP:02; imputation accuracy in Europeans is 96.5% at posterior probability ≥0.7, which we applied, setting lower-confidence calls to missing.
Childhood antibiotic exposure was participant-reported: “During childhood or as a teenager did you receive long-term or recurrent courses (three or more per year) of antibiotics (for example for tonsillitis or acne)?” Responses were coded yes, no or missing. Among participants with ≥1 valid registration in linked primary care records, we validated self-report by comparing “yes” vs “no” responders on antibiotic prescription count, estimated antibiotic-days, common bacterial infection episodes, and antibiotic prescribing adjusted for infection rates. Because primary care data were not available for most participants during childhood (<18 years), later-life records were used to proxy childhood antibiotic exposure. Prior studies show antibiotic use is correlated across the life course [3,4]. The observation window began at the earliest electronically captured prescription record (to avoid back-dated diagnoses and pre-electronic-data registration dates) and ended at the last available primary care diagnosis/prescription date or UK Biobank recruitment. Outcomes were modelled as rates per person-year using negative binomial regression with log-person-years offset, adjusted for year of birth, sex, and Townsend deprivation index; estimates were presented as incidence rate ratios (IRRs). AxSpA was defined using linked hospital (ICD-10 M45* or M081) and/or primary care codes (Read N100., N11F., N0450, X701x, X7023, X7024, or XabRZ). Acute anterior uveitis was prespecified as a positive control outcome; psoriasis and psoriatic arthritis were prespecified negative controls. Primary analysis used logistic regression to estimate odds ratios (ORs) for axSpA comparing exposed vs unexposed, adjusted for age at recruitment and sex. Sensitivity analyses additionally adjusted for recruitment centre, top 10 genetic principal components, Townsend deprivation index, childhood body size, adult BMI, maternal smoking, and personal smoking status. Missing data were handled using a missing-indicator approach and separately using multiple imputation.
Results: Analyses included 11,611 White European HLA-B27:05–positive participants. AxSpA was present in 227 (2.0%). Prolonged/recurrent childhood antibiotic use was reported by 1,481 (13%); 9,047 (78%) reported no; 1,083 (9.3%) were missing.
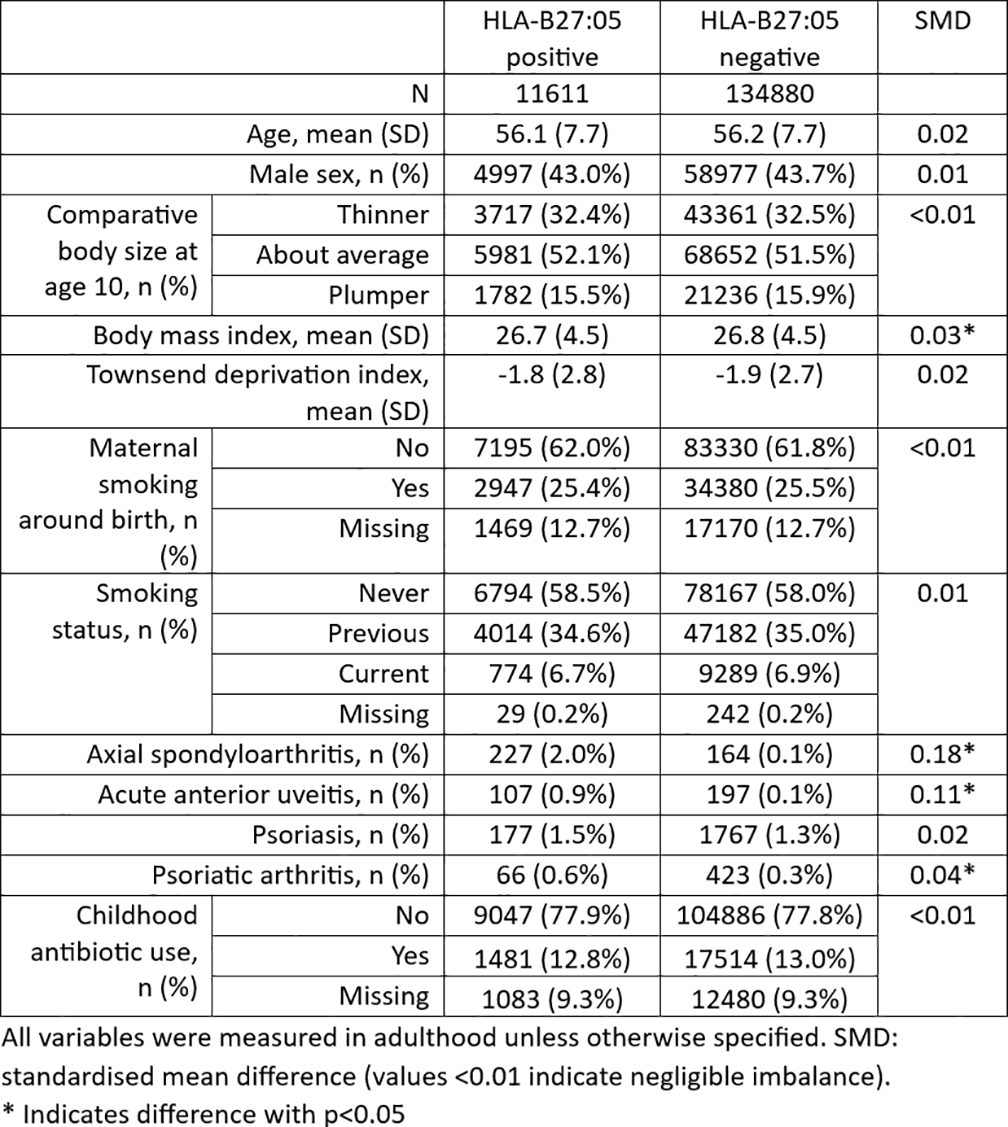
In linked primary care data (n=57,416), “yes” responders had higher antibiotic prescribing (IRR 1.83; 95% CI 1.47-2.27; p=4.3×10 -8 ), longer antibiotic exposure duration (IRR 2.15; 1.58-2.92; p=1.3×10 -6 ), higher rates of common bacterial infections (IRR 1.58; 1.52-1.64; p=1.9×10 -127 ), and higher antibiotic prescribing even after accounting for infection rates (IRR 1.96; 1.59-2.41; p=2.2×10 -10 ). Self-reported prolonged or recurrent antibiotic use during childhood was associated with approximately two-fold higher odds of axSpA among HLA-B27:05 carriers (OR 2.02; 1.42-2.89; p=1.1x10 -4 ), adjusted for age at recruitment and sex. The association was materially unchanged after additional covariate adjustment and to missing-data handling approaches. Antibiotic exposure was associated with the positive control acute anterior uveitis (OR 1.80, 1.07-3.03; p=0.03) but not with negative controls psoriatic arthritis (OR 0.97, 0.45-2.06; p=0.93) or psoriasis (OR 0.91, 0.57-1.46; p=0.71).
Conclusions: Among HLA-B27:05-positive individuals, self-reported long-term or recurrent antibiotic use during childhood was associated with approximately doubled odds of later AS. These findings are consistent with the hypothesis that early-life antibiotic exposure—potentially through disruption of the gut microbiome—contributes to axSpA susceptibility in genetically predisposed individuals. Mechanistic studies integrating longitudinal prescribing data, microbiome profiling, and immune phenotyping are needed to interrogate microbiome-mediated pathways linking HLA-B27 and axSpA. These results underscore the importance of judicious antibiotic use in childhood and may help inform future risk-stratified counselling in families with history of axSpA and known HLA-B27 carriage.
Table 1. Characteristics by self-reported long-term or recurrent childhood antibiotic exposure.
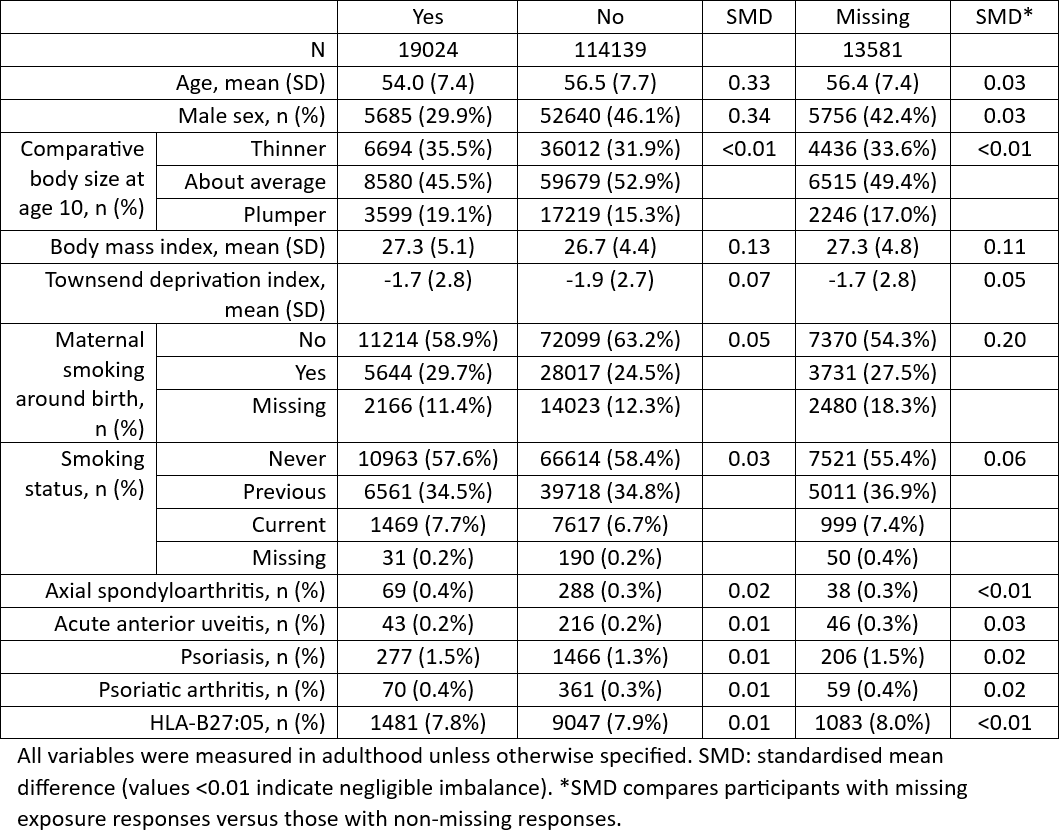
Table 2. Characteristics by HLA-B27:05 status.
REFERENCES: [1] Yang et al. Nature 2022;612:771–7.
[2] Brown et al. Res Sq (preprint) 2025;rs.3.rs-6917334.
[3] Palin et al. J Antimicrob Chemother 2019;74:2440–50.
[4] Thaulow et al. J Antimicrob Chemother 2022;77:1468–75.
Acknowledgments: NIL.
Disclosure of Interests: None declared.