fetching data ... 
Background: Remote monitoring and patient-initiated care offer flexible, patient-centered alternatives for follow-up in chronic rheumatic diseases, potentially improving resource utilization The ReMonit trial compared these follow-up strategies in patients with axSpA, and found them to be non-inferior to usual care regarding disease activity, safety, and patient satisfaction [1]. Their cost-effectiveness, however, remains uncertain.
Objectives: To evaluate the cost-effectiveness of remote monitoring, patient-initiated care and usual care.
Methods: An 18-month, three-arm non-inferiority randomized controlled trial (ReMonit, NCT050317) included patients with axSpA in low disease activity or inactive disease on stable treatment with tumor necrosis factor-inhibitor [1]. Participants were randomized (1:1:1) to remote monitoring (monthly digital self-reporting), patient-initiated care (no scheduled visits or remote monitoring), or usual care (regular visits every 6 months). All had baseline and end-of-study consultations with a rheumatologist, with additional visits available on request.
We estimated total healthcare costs over 18 months, including primary and specialist care, prescriptions, telephone follow-up, and patient travel costs. We also estimated societal costs which included healthcare costs and productivity loss (sick leave, work assessment allowance, disability). Most data on costs were obtained by linkage with national registers, Norwegian patient registry, Municipal patient registry and Norwegian prescriptions registry. Use of non-prescribed medication and travel distance were reported by participants during the trial. Telephone follow-up was registered in study records. Costs were valued in 2023 NOK. Costs from 2021 and 2022 were inflated using the Norwegian Consumer Price Index (factors: 1.116 for 2021, 1.055 for 2022). Costs were finally converted to Euros (€) using an exchange rate of 10.7433 NOK/€. Quality-adjusted life years (QALYs) were derived from EQ-5D-5L at baseline, 6, 12, and 18 months. The formal cost-effectiveness analysis was restricted to the expanded healthcare perspective. Mean costs and QALYs were estimated with generalized linear models, and follow-up strategies were ranked by effectiveness. The follow-up strategy with higher expected cost and lower expected effect than the next most effective were interpreted as a dominated strategy and was excluded from the cost-effectiveness frontier. When the cost-effectiveness frontier was established, the ratio of incremental cost to incremental QALYs (ICER) was calculated and compared to the willingness-to-pay (WTP) threshold per QALY, where the Norwegian WTP threshold of NOK 275 000 (€23 650) per QALY was applied. Uncertainty was addressed using non-parametric bootstrapping nested within the multiple imputation procedure. A total of 2,000 bootstrap replications were drawn from each of the 100 imputed datasets. The final analysis was based on pooled, bootstrapped cost-QALY pairs, and cost-effectiveness acceptability curves were constructed to illustrate the probability of each strategy being cost-effective across varying WTP thresholds.
Results: Of 243 patients enrolled, 235 completed the study: remote monitoring (n=75), patient-initiated care (n=79), and usual care (n=81).
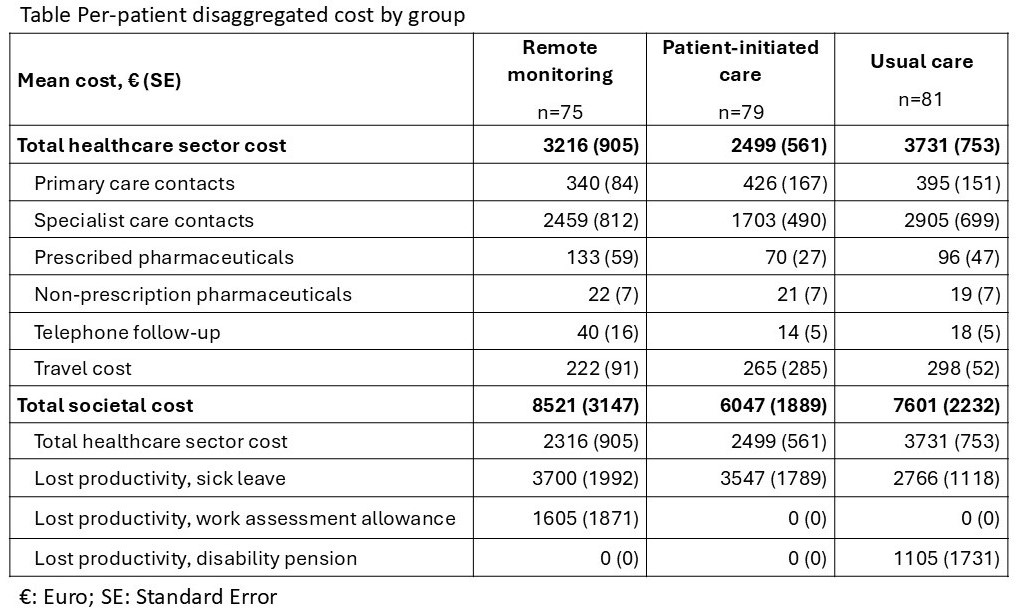
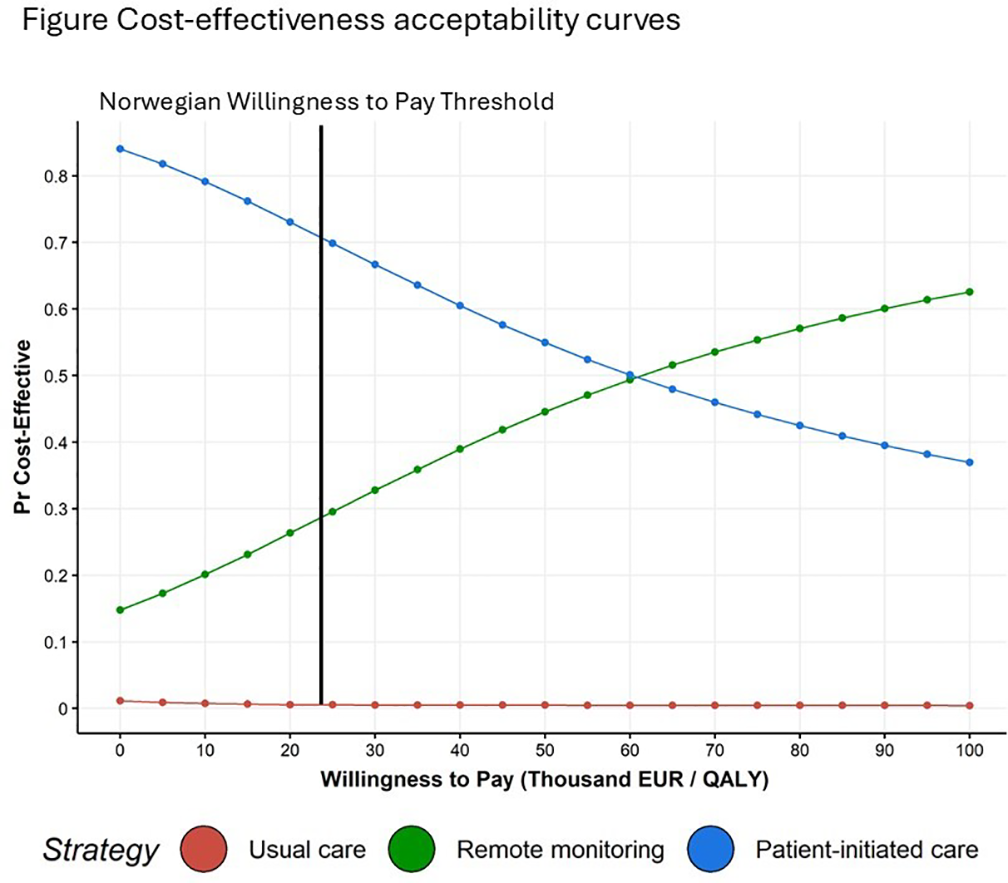
The mean healthcare costs per patient were highest in the usual care (€3 731) followed by remote monitoring (€3 216) and patient-initiated care (€2 499). Mean societal cost was highest in remote monitoring (€8 521) and usual care (€7 601), and lowest in patient-initiated care (€6 047) (Table 1). The mean QALYs gained were slightly higher with remote monitoring (1.385, 95% CI: 1.353-1.394), than with patient-initiated care (1.373, 1.370-1.400) and usual care (1.363, 1.340-1.384). Usual care incurred the highest costs and had the lowest QALYs. The incremental cost of remote monitoring vs. patient-initiated care was €775, with an incremental gain of 0.012 QALYs, giving an ICER of €60 541. Although remote monitoring achieved the highest QALYs, it was not cost-effective given the Norwegian WTP threshold of €23 650. Patient-initiated care emerged as the most cost-effective follow-up strategy. Cost-effectiveness acceptability curves were generated using bootstrap analyses, illustrating the probability of each strategy being cost-effective across varying WTP thresholds (Figure 1). At the Norwegian WTP threshold of €23,650, patient-initiated care demonstrated approximately a 70% probability of being cost-effective, whereas remote monitoring showed less than a 30% probability at the same threshold.
Conclusions: Patient-initiated care was the most cost-effective follow-up strategy of patient with axSpA in low disease activity and stable treatment. Combined with previous evidence of non-inferiority in terms of disease activity, safety, and patient satisfaction, these results support the implementation of patient-initiated care in this patient population.
Table 1.
REFERENCES: [1] Berg IJ, Kristianslund EK, Tveter AT, et al. Remote monitoring or patient-initiated care in axial spondyloarthritis: a 3-armed randomised controlled noninferiority trial. Annals of the Rheumatic Diseases 2025;84(7):1140-50. doi: 10.1016/j.ard.2025.04.019
Acknowledgments: NIL.
Disclosure of Interests: Inger Jorid Berg: None declared, Lars Asphaug: None declared, Eirik Klami Kristinaslund: None declared, Anne Therese Tveter: None declared, Laure Gossec AbbVie, Amgen, Bristol Myers Squibb, Celltrion, J&J, Eli Lilly, MSD, Novartis, Oruka, Pfizer, Takeda, UCB, AbbVie, Biogen, Eli Lilly, Novartis, UCB, Gary Macfarlane UCB, Sella Aarrestad Provan: None declared, Emil Thomassen: None declared, Annette de Thurah: None declared, Espen Haavardsholm: None declared, Siri Lillegraven: None declared, Nina Osteras: None declared