fetching data ... 
Background: Inflammatory myopathies (IM) are autoimmune diseases characterized by chronic skeletal muscle inflammation and weakness. Many IM patients feature persistent impairment in exercise capacity despite achieving remission or low disease activity with immunosuppressants. Reduced exercise capacity is associated with fatigue, increased disability and mortality. Combined resistance and endurance exercise (REE) has been reported to improve exercise capacity [1]. However, i) these landmark results, obtained in a randomized controlled trial of 23 patients, have not been replicated, ii) the training program was conducted in a hospital setting limiting patients’ access to the care, iii) the mechanism underlying the efficacy of exercise in IM has been scarcely investigated.
Objectives: This study aimed to validate the efficacy and safety of REE in patients with low disease activity IM, to compare hospital-based and community-based training programs and explore the underlying mechanisms.
Methods: Eighty patients with IM (2017 ACR/EULAR criteria) with a disease duration >12 months, CK serum levels <500 IU/L and stable medication for ≥ 6 months were prospectively included for a 36-session REE. Patients with IBM were not included. The program consisted of 30 min of aerobic exercise at 70% of VO 2 max followed by 20 min of resistance exercise at 30–40% of max strength; 3 sessions per week for 12 weeks [1]. Participants living within 50 km of the university hospital trained at this center under specialist supervision (hospital-based, HB), while others trained with a local physiotherapist guided by written specialist instructions (community-based, CB). Adherence to the program, myositis activity, exercise capacity, muscle strength, patient-reported outcomes, body composition, IMACS damage scores, and mitochondrial respiration in PBMCs scores were recorded at baseline and after completion of the 36 sessions.
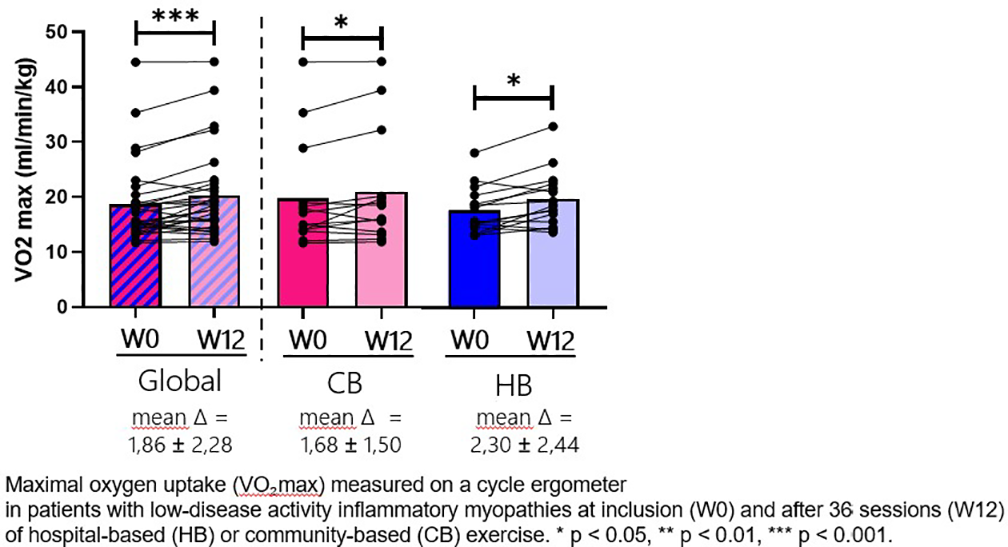
Results: At the time of this interim analysis, of the 80 eligible patients contacted, 28 remain on the waiting list as the study is still ongoing. Among the 52 patients who completed the selection visit, 5 declined to enter the program for personal reasons. Of the 47 patients who entered the protocol, 10 discontinued for various reasons (5 due to hospitalization related to comorbidity, 2 because the program was judged too time-consuming, 1 due to lack of access to a physiotherapist, and 2 for personal reasons). Twelve patients are still participating in the program and have not yet completed it. Overall, this yields a feasibility of 79%. Twenty-five patients completed the protocol (60% female; 59.7±17 years old; 12.6 ± 5.9 years disease duration) including necrotizing myopathy (n=8), scleromyositis (n=7), antisynthetase syndrome (n=4), dermatomyositis (n=4), and polymyositis (n=2). All patients were on immunosuppressive therapy, with stable doses for ≥ 6 months prior to the protocol and throughout its duration. Age, sex ratio, IM subtypes, medication, disease duration and activity did not differ between the HB and CB groups. At inclusion, mean CK was 154 ± 182 U/L, and physician VAS was 2.0 ± 0.8, which remained unchanged after completion of the protocol (respectively, 174 ± 196 U/L and 1.3 ± 1.0). VO 2 max increased to a similar extent after both the HB (Δ=1.68±1.50 mL/min/kg, p =0.0098) and CB (Δ=2.30±2.44 mL/min/kg, p =0.0033) REE (Figure 1). Power at VO 2 max (HB Δ=17.89±10.55 W, p <0.001; CB: Δ=14.93±7.38 W, p <0.001), strength evaluated by hand-held dynamometer (HB: Δ=14.43±14.48 kgf, p=0.008; CB: Δ=9.05±13.32 kgf, p=0.019), 6-min walk distance (HB: Δ=28.64±33.78m, p=0.018; CB: Δ=30.43±54.52m, p=0.057) were similarly improved in both groups. Perceived fatigue (PROMIS7) decreased in the HB (Δ=–5.±1.52, p=0.002) as well as in the CB (Δ=–5.75±1.26, p<0.001). Perceived disability (PROMIS20) decreased in the HB (Δ=–5.23±1.6, p =0.006), but not in CB (Δ=–0.38±1.31, p =0.95). REE had no impact on body composition and IMACS muscle damage score. PBMCs mitochondrial respiration improved as shown by complex IV activity (Δ=11.05± 23.72 pmol/s/10 6 cells, p =0.007). A patient developed shoulder tendinitis that resolved after medical treatment and rehabilitation. No other adverse event was recorded.
Conclusions: In both hospital-based or community-based settings, REE is feasible, safe and effective for low disease activity IM patients. Improvement of exercise capacity, muscle strength, perceived disability, and fatigue were associated with an improvement in mitochondrial respiratory capacity that may play a role in the efficacy of this non-pharmacological treatment.
REFERENCES: [1] Alemo Munters et al. Arthritis Res Ther. 2013 Aug 13;15(4):R83.
Acknowledgments: NIL.
Disclosure of Interests: None declared.