fetching data ... 
Background: In the course of rheumatoid arthritis (RA) development, the production of autoantibodies, such as rheumatoid factors (RF) or anti-citrullinated protein antibodies (ACPA), typically precedes clinical onset. However, some individuals with these autoantibodies remain asymptomatic or with arthralgia. Currently, no established methods exist to distinguish those who will progress to RA (pre-RA) from those without clinical arthritis in the early stages.
Objectives: This study aimed to elucidate the underlying genetic architecture that drives seropositive individuals towards development of RA.
Methods: We explored predictors of pre-RA, using UK Biobank as the discovery cohort and Japanese patients from Tokyo Women’s Medical University (TWMU) as the validation cohort. In UK Biobank, we identified patients with RA defined by codes M05 (seropositive RA) or M06 (other RA). Among these, patients with M05 and those with M06 who had a positive RF measurement were classified as seropositive RA (SPRA). Participants without a diagnosis of rheumatic diseases and who denied having RA in the follow-up questionnaire were classified as non-rheumatic disease (non-RMD) controls. Those with positive RF measurements but without RA were classified as asymptomatic RF positive (asy-RF). SNP array data with imputation using Genomics England panel [1] and imputed HLA aleles [2] were utilized. About ethnicity, we used information on genetically confirmed European ancestry and genotyping quality control (QC) provided by UK Biobank. At TWMU Hospital, ACPA-positive individuals without clinical arthritis were followed, and those who eventually developed RA were retrospectively classified as pre-RA. SNPs were genotyped using Asian SNP Array and subsequently imputed. HLA genotyping was performed based on whole genome sequencing. The associations of sex, smoking history, and HLA were analyzed using multivariate logistic regression in UK Biobank samples. Imputed HLA dosages were aggregated as the sum of previously reported RA-associated allele groups: HLA-A Asn77, HLA-B Asp9, HLA-DRB1 Phe9, and the amino acid sequences at positions 11, 71, and 74 of HLA-DRB1. Associations with RA, SPRA, SPRA compared to asy-RF (SPRA vs. asy-RF) were tested in European participants and non-European ones. We constructed polygenic scores (PGS) for RA, SPRA, and SPRA vs. asy-RF using PRSice2 [3], LDpred2 [4], Lassosum2 [5], and for RA and SPRA, PRS-CSx [6]. For RA and SPRA, summary statistics from external multi-ancestry GWAS [7] were used as prior weights. For the SPRA vs. asy-RF comparison, data from multi-ancestry GWAS of SPRA were employed in PRSice2. Sex, smoking history, the top 10 genomic principal components, and HLAs were included as covariates. Also, we generated logistic regression models for each phenotypes using sex, smoking history, HLAs, and one of the corresponding PGS.
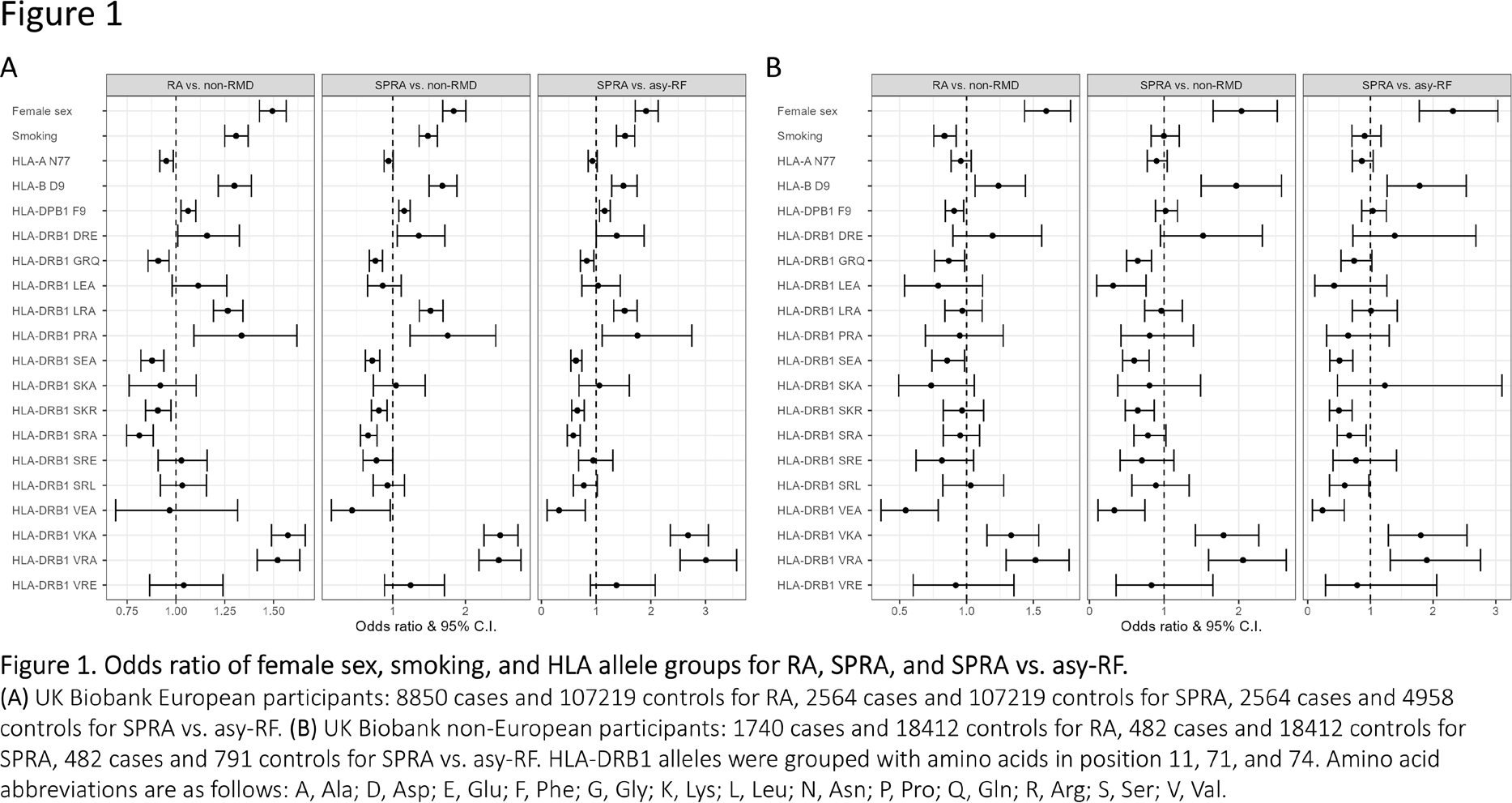
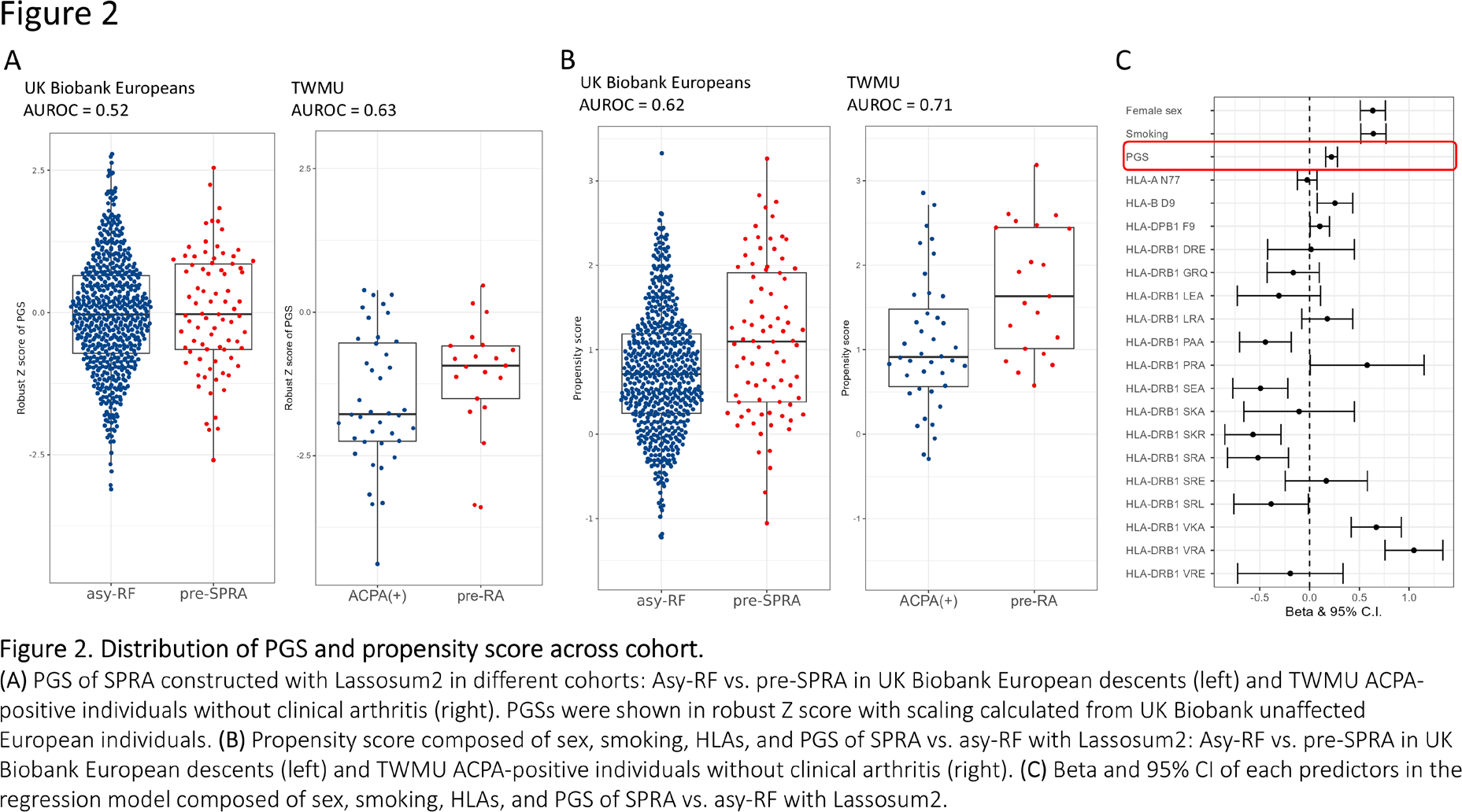
Results: We identified 13,607 RA cases and 153,702 non-RMD participants. Of these, 10,685 RA cases and 126,299 non-RMD met the criteria for genotyping QC. After reserving 95 pre-RA cases and 668 asy-RF controls for the test cohort, 8,850 RA cases and 107,219 non-RMD controls of European descent remained. We observed that HLA allele groups known to confer risk for RA had significant effects in SPRA vs. asy-RF comparison. Notably, the allele groups including the classical shared epitope, HLA-DRB1 Val11-Lys71-Ala74, and HLA-DRB1 Val11-Arg71-Ala74 exhibited the highest odds ratios of 3.00 (95% CI [2.53, 3.57]) and 2.68 (95% CI [2.36, 3.05]), respectively, exceeding those of female sex (1.91, 95% CI [1.71, 2.13]) and smoking (1.53, 95% CI [1.37, 1.71]) (Figure 1A ). The strong effects of these allele groups were also observed in the comparison of SPRA vs. asy-RF among non-European participants (Figure 1B ). Indeed, in TWMU cohort of 21 ACPA-positive pre-RA cases and 40 asymptomatic ACPA-positive controls, the allele frequency of HLA-DRB1 Val11-Arg71-Ala74 was higher in cases (11/42 vs. 9/80, p = 0.04). The common variant PGS for SPRA vs. asy-RF developed using Lassosum2 was the most effective predictor of pre-RA within ACPA-positive individuals in TWMU, with an AUROC of 0.63, but its AUROC was 0.52 for pre-RA prediction in UK Biobank (Figure 2A ). Logistic regression model with with PGS for SPRA vs. asy-RF constructed using Lassosum2 yielded maximum AUROC of 0.71 in TWMU cohort (Figure 2B ). PGS had significant weight (β = 0.22, p = 0.0002) in this model (Figure 2C ).
Conclusions: In this study, we demonstrated that specific HLA allele groups are critical risk factors for the transition from seropositivity to SPRA. This finding was consistent across populations. The common variant PGS alone was insufficient to stratify high-risk pre-RA individuals from those without clinical RA. Furthermore, the PGS that performed better in European populations did not do so in East Asian participants, and vice versa. A multivariate model combining sex, smoking, HLA, and PGS showed improved predictive performance, with PGS playing a significant role in this combined model. These results emphasize the necessity of incorporating multiple predictors, such as HLA, PGS, and potentially other omics data.
REFERENCES: [1] Shi, S. et al. Nat Genet 56, 1800–1803 (2024).
[2] Bycroft, C. et al. Nature 562, 203–209 (2018).
[3] Choi, S. W. & O’Reilly, P. F. Gigascience 8, giz082 (2019).
[4] Privé, F., Arbel, J. & Vilhjálmsson, B. J. Bioinformatics 36, 5424–5431 (2021).
[5] Privé, F., Arbel, J., Aschard, H. & Vilhjálmsson, B. J. Human Genetics and Genomics Advances 3, 100136 (2022).
[6] Ruan, Y. et al. Nat Genet 54, 573–580 (2022).
[7] Ishigaki, K. et al. Nat Genet 54, 1640–1651 (2022).
Acknowledgments: NIL.
Disclosure of Interests: Taiki Yamaguchi Taisho Pharmaceutical Co., Yuko Okamoto AbbVie Japan GK, Chugai Pharmaceutical Co., Taisho Pharmaceutical Co., Tadashi Hosoya Ono Pharmaceutical Co., Ltd.; Chugai Pharmaceutical Co., Ltd.; Janssen Pharmaceutical K.K.; Bristol Myers Squibb; Asahi Kasei Pharma; GlaxoSmithKline; Eli Lilly Japan K.K.; Takeda Pharmaceutical Company Limited; Eisai Co., Ltd.; Astellas Pharma Inc.; Novartis Pharma K.K.; Daiichi Sankyo Co., Ltd.; Mitsubishi Tanabe Pharma Corporation; Pfizer Japan Inc.; AbbVie GK; Taisho Pharmaceutical Co., Ltd.; Teijin Healthcare Limited; Medical & Biological Laboratories Co., Ltd.; AstraZeneca K.K.; and Otsuka Pharmaceutical Co., Ltd., Sony Corporation, NEC, and Terumo life science foundation, Katsunori Ikari Asahi Kasei Pharma Co.; Astellas Pharma Inc.; AbbVie Japan GK; Ayumi Pharmaceutical Co.; Bristol-Myers Squibb Co.; Chugai Pharmaceutical Co., Ltd.; Daiichi Sankyo Co., Ltd.; Eisai Co., Ltd.; Eli Lilly Japan K.K.; Gilead Sciences, Inc.; Hisamitsu Pharmaceutical Co., Inc.; Janssen Pharmaceutical K.K.; Kaken Pharmaceutical Co., Ltd.; Mochida Pharmaceutical Co., Ltd.; Pfizer Japan; Taisho Pharmaceutical Co., Ltd.; Takeda Pharmaceutical Co., Ltd.; Tanabe Pharma Co.; UCB Japan Co. Ltd., AbbVie Japan GK; Chugai Pharmaceutical Co., Ltd.; Eisai Co., Ltd.; Eli Lilly Japan K.K., Chikashi Terao: None declared, Shinsuke Yasuda Otsuka Pharmaceutical Co. Ltd., Abbvie Japan Co., Ltd., AsahiKASEI Co., Ltd., Astrazeneca, Chugai Pharmaceutical Co., Ltd., Eli Lilly Japan K.K., Mitsubishi-Tanabe Pharma Co.Ltd., Ono Pharmaceutical Co. Ltd. Otsuka Pharmaceutical Co. Ltd., Stratoimmune Co. Ltd., Chugai Pharmaceutical Co., Ltd., ImmunoForge, Novartis Pharmaceutical Co. Ltd., AsahiKASEI Co., Ltd., Yuta Kochi Daiichi Sankyo, Inc.