fetching data ... 
Background: Sjögren’s Disease (SjD) is a systemic autoimmune disease with a wide range of clinical and molecular phenotypes, making early diagnosis and treatment challenging. The hallmark clinical features of chronic dry eyes and mouth result from lymphocytic infiltration of the exocrine glands and subsequent glandular dysfunction and destruction. Improved delineation of the pathophysiological processes in the salivary gland is foundational to understanding the underlying mechanisms of disease. Xenium In Situ spatial transcriptomics uses subcellular mapping of transcripts for single cell deconstruction of tissue. In this study, Xenium was used to explore differences in the salivary gland from SjD case that are negative or positive for the hallmark anti-Ro/SSA autoantibody and/or lymphocytic infiltration of the salivary gland.
Objectives: Use Xenium In Situ to define the spatial transcriptomic architecture of salivary gland across SjD subphenotypes to identify cell-type-specific pathogenic signatures of early disease.
Methods: IRB approval was obtained. Spatial transcriptomics was performed on n=53 salivary gland biopsies using the Xenium In Situ platform (10x Genomics). The cohort was stratified by clinical diagnosis (SjD vs. Healthy Control [HC]), anti-Ro/SSA antibody status (Ro+ or Ro-), and histological focus score (FS) - a standard histological marker of lymphocytic aggregation in the gland. Samples were grouped as follows: HC with FS < 0.25 (HC FS-, n=5), HC with FS ≥ 0.25 (HC FS+, n=4), Ro- SjD with FS ≥ 1 (SjD Ro-, FS+, n=16), Ro+ SjD with FS < 1 (SjD Ro+, FS-, n=4), and Ro+ SjD with FS ≥ 1 (SjD Ro+, FS+, n=24). A stringent quality control (QC) workflow was applied to the initial dataset of 1.16 million cells to ensure high-fidelity spatial analysis. Cells were filtered based on nuclear presence and integrity of cell segmentation. Cells lacking a detectable DAPI-stained nucleus and those identified with segmentation artifacts, such as erroneous boundaries resulting in “multinucleated” cell objects in high-density inflammatory regions, were excluded. Resulting refined dataset of 1.01 million cells was used for downstream analyses. Pseudo-bulk differential gene expression (DGE) was performed to identify cell type-specific transcriptional alterations across the subphenotypes. Transcript counts were aggregated for each cell type at the individual sample level to create a representative expression profile that accounts for inter-sample biological variability, then DESeq2 was used to identify differentially expressed genes (DEGs): adjusted p-value (padj) < 0.05 and log2 fold-change (log2FC).
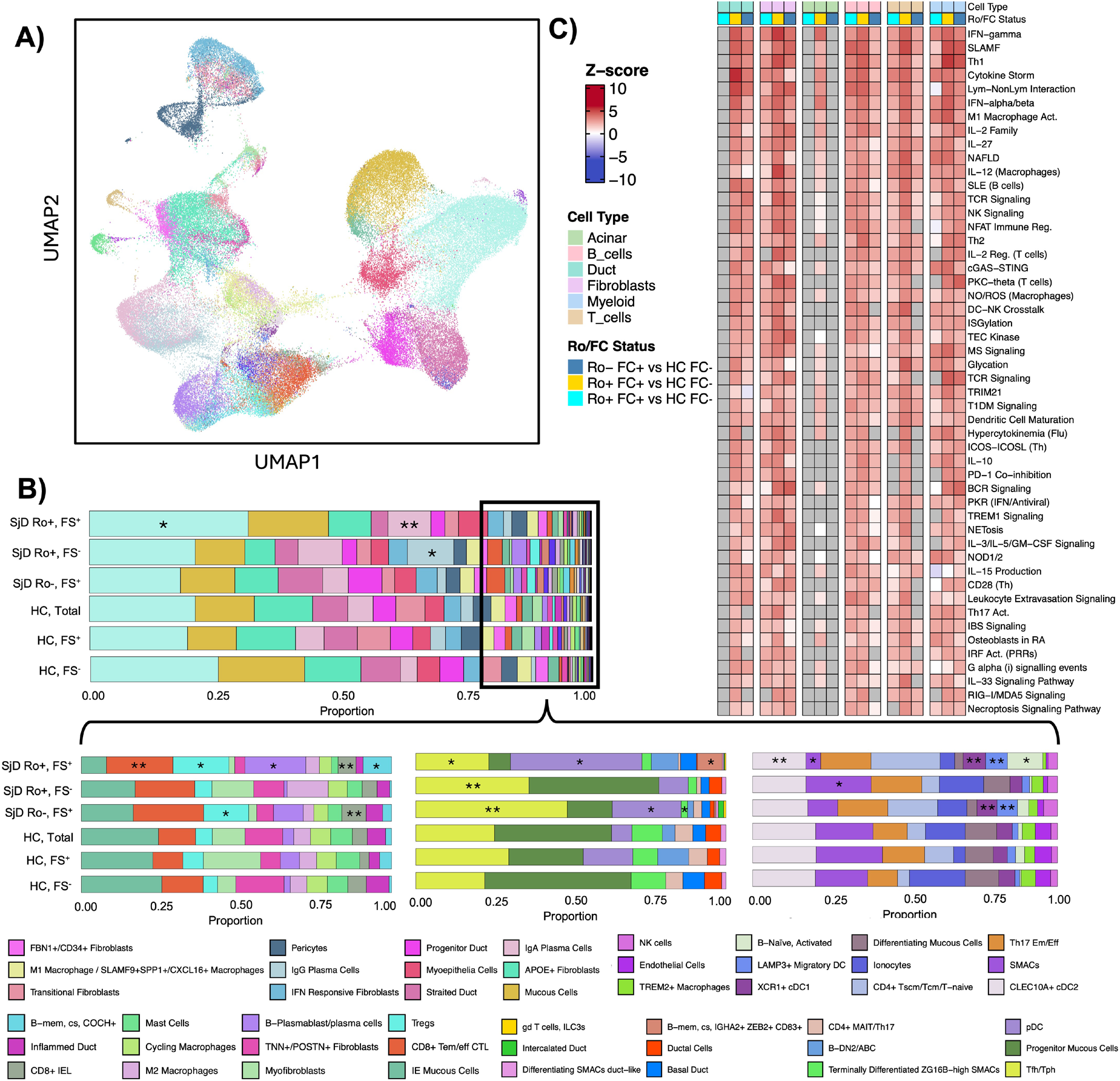
Results: Xenium spatial profiling resolved 1.01 million cells into a high-resolution salivary gland atlas with distinct clusters across three major cell types: epithelial (e.g., Inflamed/Progenitor Ducts), Mesenchymal (IFN-responsive Fibroblasts), and immune subsets (e.g. B-DN2/ABC, Tfh/Tph, and IgG+ Plasma cells). This granular mapping captured the complex cellular heterogeneity of the gland and provided a spatial framework to distinguish early pathogenic signatures across SjD subphenotypes. DGE magnitude was synergistically driven by Ro status and FS, with the most profound shifts occurring in B cells (895 DEGs) and T cells (605 DEGs) in Ro+ cohorts (FS > 1) compared to HC FS-. Notably, high FS was a primary driver of dysregulation such that Ro+ FS- samples (FS < 1) showed minimal shifts while Ro- FS+ retained significant signals, particularly in lymphocytes. Cell proportion percentage plot displays cellular composition across subsets. Ro+ FS+ showed marked T and B cell expansion, while Ro- was dominated by macrophages, fibroblasts, and DCs. Overlap between Ro+ FS- and Ro- groups, alongside acinar/ductal shifts, underscores the distinct immune-epithelial landscapes in SjD. Substantial dysregulation was also observed in stromal (fibroblasts: 249 DEGs) and epithelial (acinar: 261 DEGs) compartments in inflamed tissues, while ductal cells showed unique sensitivity in the Ro- FS+ subgroup. Ingenuity Pathway Analysis (IPA) of distinct comparisons across B cells, T cells, acinar, and duct cells, stratifying cases by Ro status and FS (FS±) against HCs, revealed robust activation of IFN-gamma, alpha/beta, and Th1 pathways. This activation was most prominent in Ro+ and FS+ subgroups. Enriched BAFF/BCR signaling in B cells and SLAMF-mediated crosstalk underscore systemic immune dysregulation and highlight cell-specific interferon signatures central to SjD pathogenesis.
Conclusions: Our study established a high-resolution spatial atlas of salivary gland tissues in health and SjD. Pathogenic transcriptomic dysregulation was observed in Ro- SjD cases, characterized by epithelial stress ( KRT16 , IDO1 ) and inflammatory signaling ( IRF1 , CXCL10/11 ) within B and T cell compartments. While dysregulation exists in Ro- patients, dysregulation was more pronounced in Ro+ patients, marked by intense B cell recruitment ( CXCL13 ) and widespread IFN-stimulated gene expression across all compartments. These findings illustrate that spatial transcriptomics can resolve the cellular architecture of salivary gland and identify markers of molecular and cellular dysregulation in subphenotypes of SjD.
Analysis of 10X Xenium data from minor salivary glands (MSG; n=53) biopsied from Sjögren’s Disease (SjD) and healthy control (HC) individuals detected 1,011,721 cells and 61 cell types. (A,B). SjD cases were separated by Ro autoantibody status (Ro+ or Ro-) and Focus score (larger or smaller than 1), then case-control differential expression (DE) across cell types were analyzed using a pseudo-bulk approach. Significant DE transcripts were analyzed using Ingenuity Pathway Analysis to identify disease- and sub-phenotype-specific pathway dysregulation (C) Heatmap shows the top 50 significantly dysregulated pathways.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Songyuan Yao: None declared, Marcin Radziszewski: None declared, James Li: None declared, Cherilyn Pritchett Frazee: None declared, Mandi M Wiley: None declared, Kandice L Tessneer: None declared, Matthew Caleb Marlin Received consulting fees from Standard Biotools, Miles Smith: None declared, Kevin Wei: None declared, Soumya Raychaudhuri: None declared, Michael Brenner: None declared, Lam Tsoi: None declared, Johann E Gudjonsson: None declared, Nir Hacohen: None declared, Judith A. James Received consulting fees from GSK, Received research support from Progentec Biosciences, R Hal Scofield Advisory Board Member for Janssen Pharmaceuticals, IQVIA, Received consulting fees from Johnson and Johnson Innovative Medicine (formerly Janssen) and Merk Pharmaceuticals, Astrid Rasmussen Current affiliation: Boston Children’s Hospital, Received consulting fees from Immunovant Clinical Outcomes Solutions, Stephen Shiboski: None declared, Bhuwan Khatri: None declared, Alan Baer Received consulting fees from Bristol Myers Squibb (BMS), A. Darise Farris Grant/research support from Johnson and Johnson Innovative Medicine (formerly Janssen; ended 12/31/2023), Caroline Shiboski Received consulting fees from BMS, Joel M Guthridge: None declared, Blake M Warner Active research agreements with Astellas Bio, Pfizer, Christopher J Lessard Received consulting fees from Johnson and Johnson Sjögren’s Disease Advisory Board, Grant/research support from Johnson and Johnson Innovative Medicine (formerly Janssen; ended 12/31/2023).