fetching data ... 
Background: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a rare and severe autoimmune disease, characterized by a pauci-immune necrotizing vasculitis leading to inflammation and damage of major organs. Case reports suggest that viral infections such as cytomegalovirus (CMV) reactivation may contribute to disease flares. Additionally, CMV reactivation during immunosuppressive therapy poses a risk of severe infections. Previously, CMV reactivation was demonstrated to occur in ~20% of AAV patients after immunosuppressive treatment [1]. A previous study demonstrated that a CMV-specific CD4 + CD28 - T cell subset is expanded in AAV patients, while valacyclovir could suppress this subset and subclinical CMV reactivation [2]. However, the phenotype and clonal architecture of CMV-specific T cells in AAV at single-cell resolution remain incompletely defined.
Objectives: Our study aims to precisely characterize the phenotype and clonality of CMV-specific T cells in AAV patients to get more insight into the role of CMV in the pathophysiology of AAV.
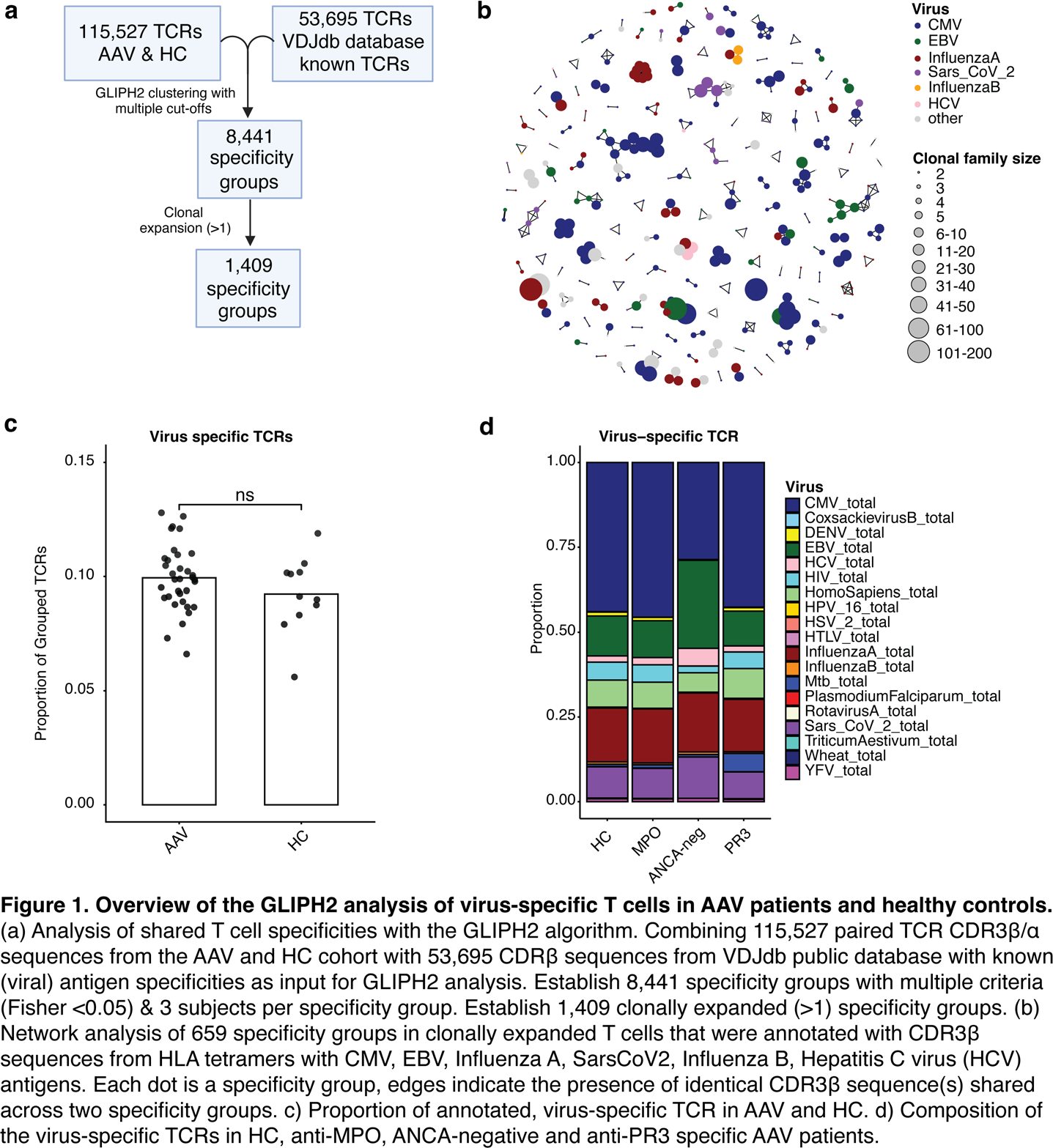
Methods: Single cell RNA and T cell receptor (TCR) sequencing combined with CITE-seq staining was performed of isolated T cells from anti-MPO (myeloperoxidase) (n=9), anti-PR3 (proteinase-3) (n=9) and ANCA-negative (n=1) AAV patients and aged-matched healthy controls (HCs) (n=11). GLIPH2 (Grouping of lymphocyte interactions by paratope hotspots) algorithm was used to cluster T cell receptors (TCRs) that recognize the same epitope. 115,527 paired TCR CDR3β/α sequences from all AAV patients and HC were analyzed with GLIPH2 in combination with 53,695 CDR3β from the VDJdb public database with known (viral) antigen specificities (Figure 1a). The specificity groups were determined with a Fisher score <0.05 and at least 3 different subjects per group. Next, the specificity groups were annotated with known tetramer-derived virus-specific TCRs from the public VDJdb database (Figure 1b). AAV patients and HCs were HLA-typed, which was incorporated into the GLIPH2 analyses. Additionally, CMV IgG was tested to determine CMV serology status.
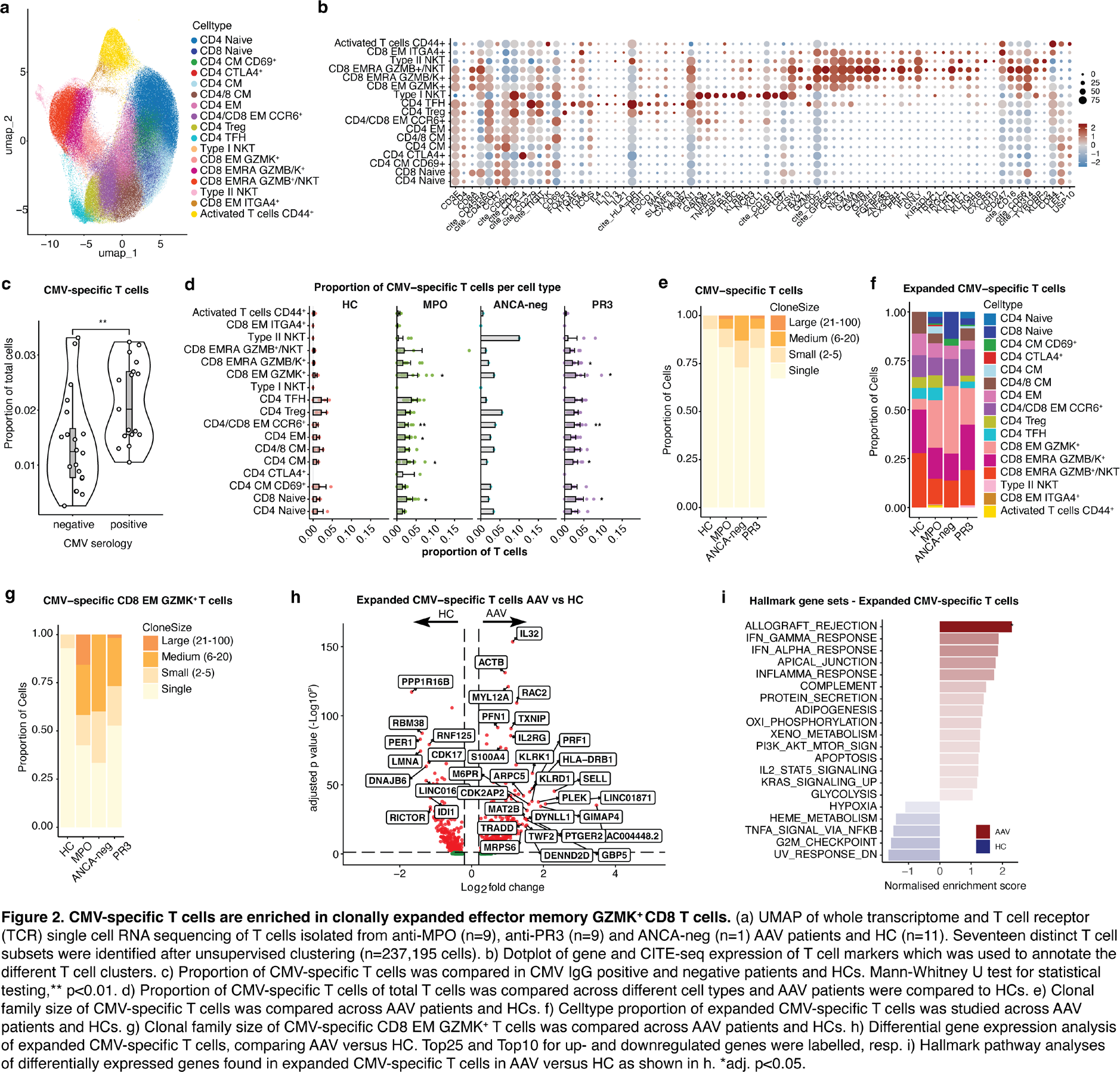
Results: In this study, we found 8,441 shared specificity groups that included 21,044 TCRs (18.2%) with the GLIPH2 algorithm (Figure 1a). 1409 specificity groups were found among clonally expanded T cells (968 TCRs) (Figure 1a-b). Overall, an average of 9.94±1.44% of AAV TCRs were virus specific, which was comparable to 9.24±1.65% in HC (Figure 1c). Also, the proportion of different virus-specific T cells was not different between AAV and HC, whereas the majority comprised CMV-specific T cells, followed by Influenza A, and EBV-specific T cells (Figure 1d). Different T cell subsets were identified after unsupervised clustering and annotated based upon gene and CITE-seq expression (n= 237,195 cells) (Figure 2a-b). CMV-specific T cells were detected in all samples to some extent, but they were significantly increased in CMV IgG positive (2.15±0.74%) compared to CMV IgG negative samples (1.39±0.86%, p=0.005) (Figure 2c). Interestingly, in both anti-MPO and anti-PR3 AAV the CMV-specific T cells were enriched in the CD8 effector memory (EM) GZMK + T cells as compared to HC (2.77±2.59%, 2.81±2.44%, 0.52±0.56%, p=0.012, p=0.011, resp.), among other subsets (CD4/CD8 EM CCR6 + , CD4 CM, CD8 naive) (Figure 2d). In contrast, this was not the case for EBV- and Influenza A-specific T cells (data not shown). In addition, CMV-specific T cells were clonally expanded in AAV patients as compared to HC (Figure 2e). Focusing on the expanded CMV-specific T cells (2 or more clones per family), we observed that the majority were CD8 EM GZMK + T cells in AAV (Figure 2f), while CD8 EMRA GZMB + clusters were enriched in all groups. Moreover, the CMV-specific CD8 EM GZMK + T cells were highly clonally expanded in AAV (Figure 2g). Differential gene expression analyses demonstrated that expanded CMV-specific T cells in AAV, when compared to HC, upregulated several genes ( PRF1, IL32, KLRD1 ) (Figure 2h), and pathway enrichment analyses showed that these genes clustered in hallmark pathways involved in allograft rejection (Figure 2i), indicating that these T cells are highly inflammatory, cytotoxic and activated.
Conclusions: Our study demonstrates that CMV-specific T cells in AAV patients are enriched in clonally expanded effector memory GZMK + CD8 T cells, which could indicate (subclinical) CMV reactivation in AAV patients. Given these findings, it may be beneficial to explore the role of CMV in the pathophysiology of AAV further.
REFERENCES: [1] Kawamori et al. 2025 Modern Rheumatology.
[2] Chanouzas et al. 2019 The Journal of Infectious Diseases.
Acknowledgments: NIL.
Disclosure of Interests: Laura S. van Dam: None declared, Mengrui Zhang: None declared, Jae-Seung Moon: None declared, Salvinaz Moutusy: None declared, Friederike Held: None declared, Shima Parsafar: None declared, Audra Horomanski I am involved with and receive research support for clinical trials from Zenas, Gilead, and Viela Bio in the past year., Orr Sharpe: None declared, Jolijn R van Leeuwen: None declared, Tobias Lanz: None declared, Cees van Kooten: None declared, Y.K. Onno Teng: None declared, William Robinson: None declared.