fetching data ... 
Background: While proteinase 3 (PR3)-anti-neutrophil cytoplasmic antibody (ANCA) IgG are routinely measured in clinical practice when assessing ANCA-associated vasculitis (AAV), PR3-specific IgA and IgM are not. Preliminary evidence suggests that IgA and IgM PR3-ANCA, taken individually, may relate more closely to disease activity or specific organ involvement, as for IgM PR3-ANCA and alveolar hemorrhage. However, little is known about whether combinations of antigen-specific Immunoglobulin (Ig) isotype positivity may confer higher severity profiles in AAV, as for rheumatoid arthritis or antiphospholipid syndrome. Yet the relationship between PR3-specific isotypes, disease activity, and clinical manifestations remains incompletely understood.
Objectives: This study aims to investigate whether combinations of PR3-specific isotype positivity (IgG, IgA, and IgM) and titers in AAV patients ever positive for PR3-ANCA are associated with disease activity and specific clinical features.
Methods: Indirect enzyme-linked immunosorbent assay (ELISA) was used for detection of IgGs, IgAs and IgMs directed against PR3, in sera obtained from PR3-ANCA positive patients and healthy donors (HD) from two centers. Only patients with a diagnosis of AAV (either granulomatosis with polyangiitis, GPA, or microscopic polyangiitis, MPA) and previous history of or current positive serology for PR3-ANCA (IgG) were included. Active patients were sampled before any treatment (with the only exception of systemic glucocorticoids). Patients in remission with disease-modifying antirheumatic drugs (DMARDs) were sampled anytime during follow-up, while patients in remission induced with rituximab (RTX) were sampled after B-cell repopulation (CD19 + ≥ 10 cells/mL). Clinical data at the time of blood draw were collected from charts. ELISA plates were coated with human conformationally intact, inactive human recombinant PR3 (rPR3). Following serum incubation, the presence of IgG, IgA and IgM antibodies was detected using an enzyme-conjugated secondary antibody specific to either human IgGs, IgAs or IgMs respectively. Data are presented as the net Optical Density values at 405 nm (Net OD 405nm ) measured after 20 minutes of colorimetric substrate reaction.
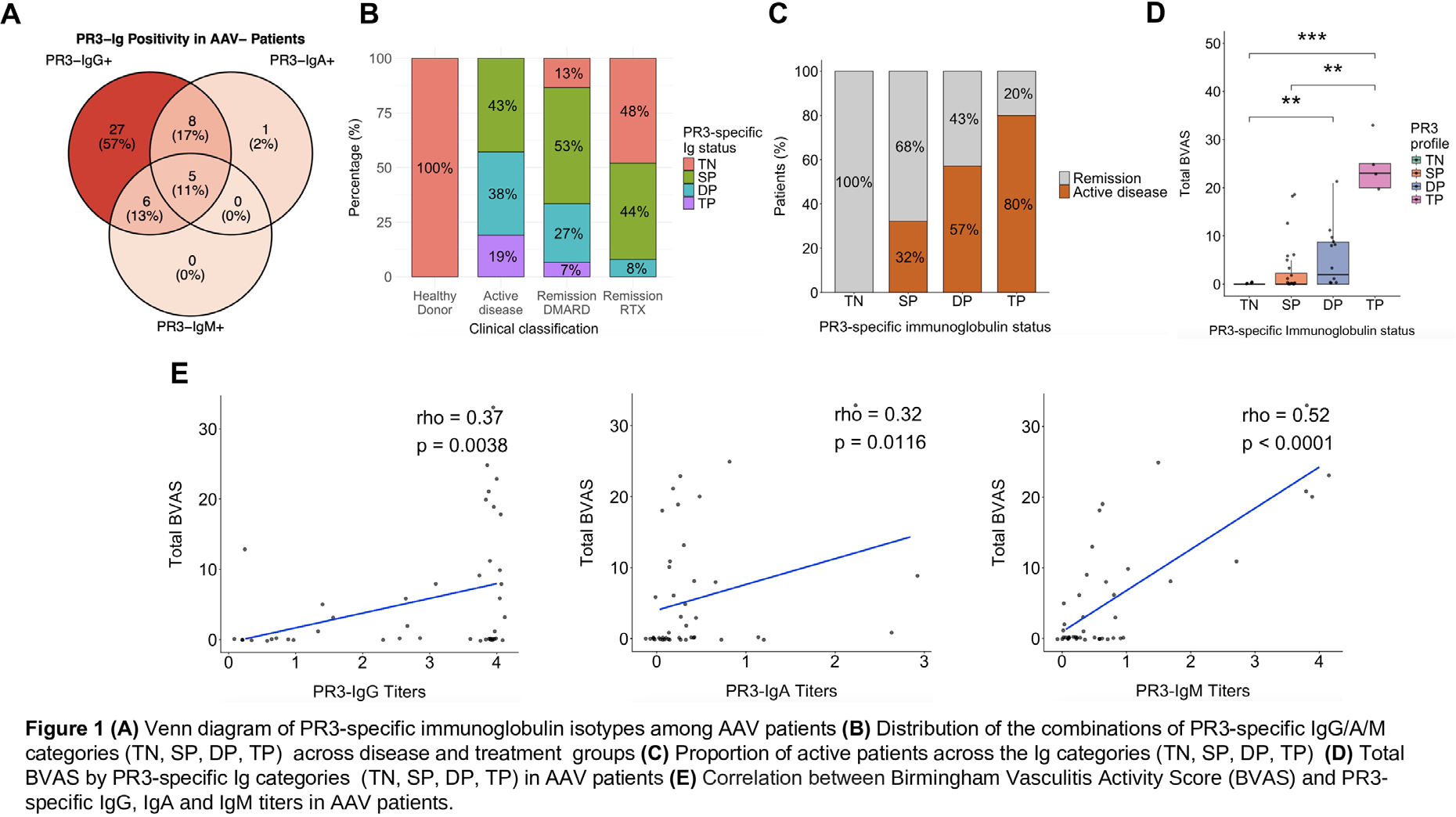
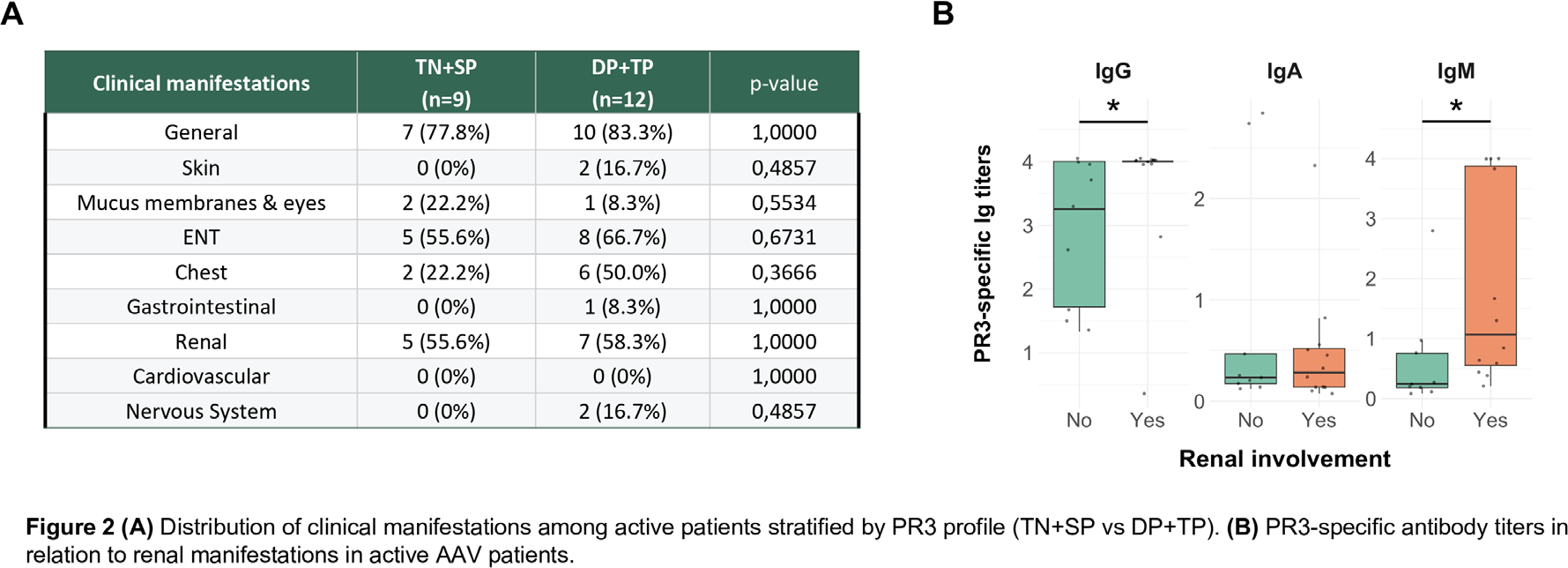
Results: Sixty-one patients previously diagnosed with PR3-ANCA AAV (56 GPA, 5 MPA; 38% female; median age 63 years [IQR 52–74]) and 20 HDs (50% female; median age 63.5 years [IQR 55.25–74.50]) were included. At the time of sampling, 21 patients (34%) had active disease, with a median BVAS of 9 [IQR 5–19]. The remaining 40 AAV patients were in remission, of which 63% had previously received RTX, and 37% were in remission under conventional DMARD therapy. Evaluation of PR3-specific Ig isotypes revealed heterogeneous serological profiles among patients. As expected, all HDs tested negative for PR3-specific IgG, IgA, and IgM, as well as 23% of AAV patients in remission (n=14, 12 after RTX and 2 under DMARDs). To investigate association between the combinations of PR3-specific positive Ig isotypes and disease activity, patients were first stratified according to their serological profile: triple negative (TN), single positive (SP), double positive (DP), and triple positive (TP). Forty-seven patients had at least one positive PR3-specific Ig ( Figure 1A ), 59% (n= 28) were SP (all IgG+ but one that was IgA+), 30% (n= 14) were DP (IgG+/IgA+ or IgG+/IgM+), and 11% (n= 5) were TP. The distribution of these profiles differed across clinical and treatment groups ( Figure 1B ). No active AAV patient was TN, whereas TP patients were observed only among active disease and DMARD-treated remission groups (19% and 7%, respectively). Disease activity, assessed using the Birmingham Vasculitis Activity Score (BVAS), was analyzed according to combinations of PR3-specific Ig isotypes. Patients classified as TN, SP, DP, and TP demonstrated a progressively increasing proportion of active disease (defined as BVAS ≥ 1; p < 0.0001, Figure 1C ), as well as higher levels of BVAS score ( Figure 1D ). DP patients exhibited higher disease activity than TN patients (p<0.01), while TP patients had the highest total BVAS compared to both TN and SP groups (p<0.001 and p<0.01, respectively). Significant correlations were observed between BVAS score and the three PR3-specific isotypes taken individually (all<0.05), with a moderate-to-strong correlation seen for IgM (Rho=0.52, p<0.001), suggesting an association between PR3-specific humoral activation and disease activity ( Figure 1E ). The stratification of the whole cohort by PR3-specific Ig isotype combinations showed no association with age groups or between sexes (p>0.05). Among the 21 active patients, comparison between the TN+SP and DP+TP groups did not reveal significant differences across clinical manifestations (p>0.05, Figure 2A ). In active AAV patients, only renal involvement was associated with higher PR3-specific IgG and IgM titers (p<0.05 for both comparisons, Figure 2B ).
Conclusions: Our findings showed a high prevalence of combinations of PR3-specific IgG, IgA and IgM positivity in AAV patients, proving correlations between multiple positivity and disease activity, and supporting the hypothesis of a possible link between a broader humoral immune activation and a higher disease activity in AAV. Furthermore, PR3-specific IgM showed the strongest correlation with BVAS and was associated with renal involvement in active patients, potentially reflecting differences in humoral immune activation among clinical subgroups. Larger studies are needed to prove the clinical utility of stratification by PR3-specific Ig isotype combinations, and determine whether this could help to predict relapse risk or disease morbidity.
REFERENCES: [1] Wiik, A. Arthritis research vol. 2,4 (2000): 252-4.
[2] Sandin, C et al. Clinical and experimental immunology vol. 184,2 (2016): 208-15.
[3] Clain, J M et al. Clinical and experimental immunology vol. 188,1 (2017): 174-181.
Acknowledgments: NIL.
Disclosure of Interests: None declared.