fetching data ... 
Objectives: To develop a deep learning model for classifying ultrasound images of salivary glands (SG) [parotid (PG) and submandibular (SMG) based on the Outcome Measures in Rheumatology (OMERACT) 0-3 semiquantitative scoring system for B-mode ultrasound-assessed parenchymal abnormalities in SG in Sjögren disease (SjD)
Methods: For training, we used 3 datasets of SG (PG and SMG) ultrasound images representative of the OMERACT scores: 1. A dataset of 225 ultrasound images acquired with different ultrasound systems of 150 SjD patients across four European centers (
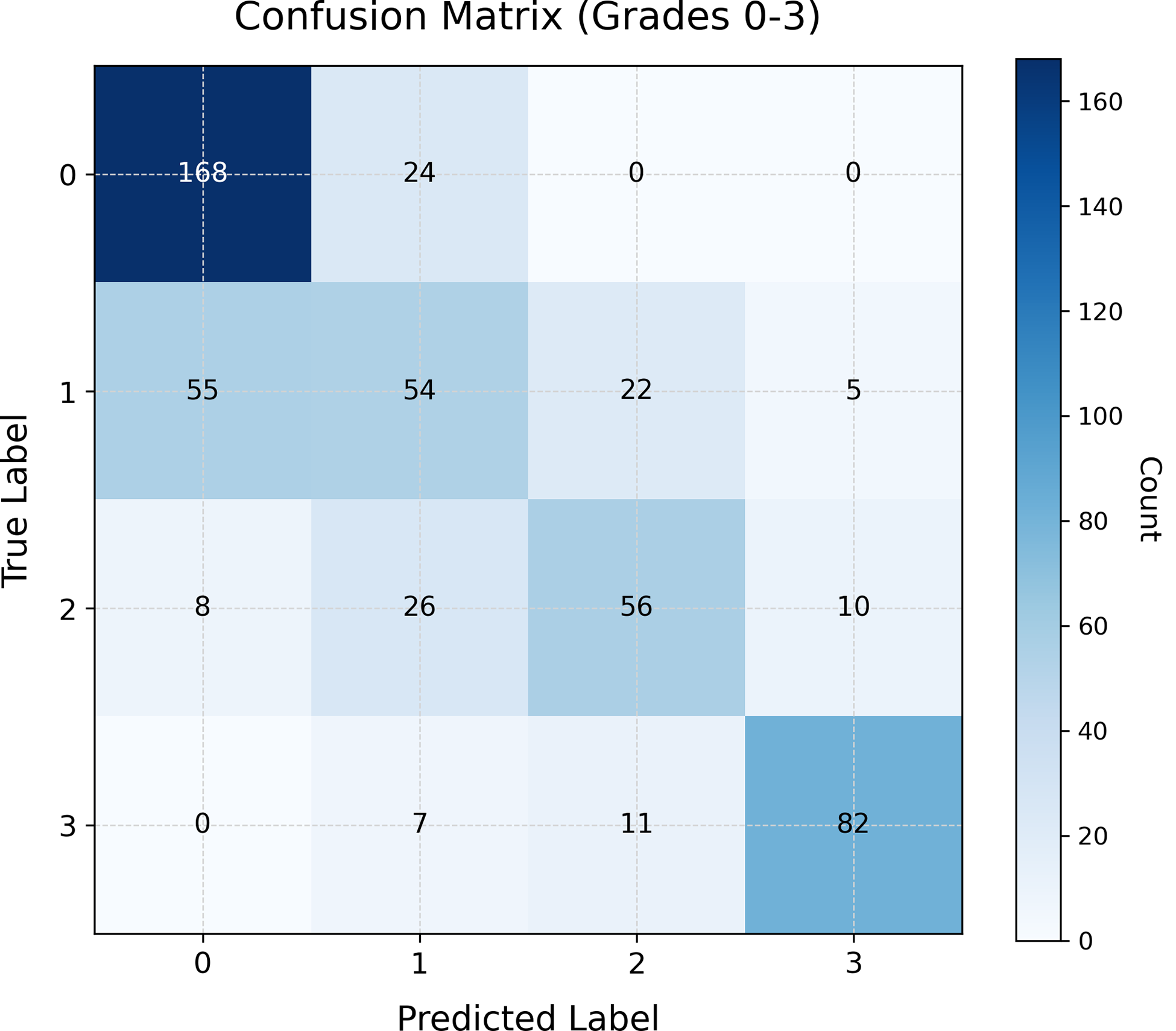
Results: The overall performance of the model for grading classes is shown in Table 1. The broad model achieved an accuracy of 88% in distinguishing between 0/1 and 2/3 grades. However, the more specific models, fine-tuned for the 0/1 and 2/3 categories, performed differently across categories: 72% accuracy for the 0/1 classification and 82% for the 2/3 classification. This reflects the increased difficulty of fine-grained classification. The confusion matrix (Figure 1) showed that the model performed well in classifying SG with grade 3 but faced challenges with intermediate categories (grade 1 and grade 2). Moreover, the network showed difficulty discriminating between grade 0 and grade 1. These findings suggest that while the broad classification was accurate, the fine-tuned models might require additional data or further optimization to improve accuracy in distinguishing between milder forms of SG involvement. The error rate by operator was 0.36 for Operator 1 and 0.32 for Operator 2. Neither the global comparison nor the class-wise analysis revealed statistically significant differences between operators. Regarding the device comparison, the mean error rate was 0.38 for the high-end ultrasound system and 0.31 for the wireless handheld ultrasound device, with no statistically significant global difference. However, when analyzed by class, a statistically significant difference was observed for grade 2 (p <0.001): the error rate was 0.74 for the high-end ultrasound system compared to 0.34 for the wireless handheld ultrasound device.
Conclusions: Our results showed the potential of deep learning models, specifically convolutional neural networks, to classify ultrasound images of SG based on the severity of parenchymal abnormalities in SjD. While the broad classification model performed very well, the fine-tuned models, which differentiate between some specific grades of SG involvement, still face challenges. Future work should include further refinement of the fine-tuned models with additional data, which allows more complex architectures, or domain-specific adjustments. Additionally, our results suggested that operator-related variability has minimal impact on classification accuracy, while device-related differences may affect performance in specific classes. Further analyses in larger datasets are needed to determine whether these findings reflect true performance differences or arise from sample variability
Accuracy/ Precision
| Precision | Recall | F1-score | |
|---|---|---|---|
| Grade 0 | 0.73 | 0.88 | 0.79 |
| Grade 1 | 0.49 | 0.40 | 0.44 |
| Grade 2 | 0.63 | 0.56 | 0.59 |
| Grade 3 | 0.85 | 0.82 | 0.83 |
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.