fetching data ... 
Background: Delays in diagnosis of juvenile idiopathic arthritis (JIA) may impact long-term disease outcomes and both physical and psychosocial aspects of health-related quality of life (HRQoL). Reported differences in incidence and prevalence of JIA by ethnic group may be associated with diagnostic delays, and variability in referral and diagnosis pathways in the UK. However, the relationship between sociodemographic factors and HRQoL remains unclear.
Objectives: This study investigated changes in HRQoL and disease activity among children and young people with JIA and the association with ethnic group and socioeconomic position in the UK.
Methods: Treatment-naive children and young people diagnosed with JIA between 2001 and 2019 were recruited at the point of diagnosis from seven UK paediatric rheumatology centres into the Childhood Arthritis Prospective Study (CAPS). Self-declared ethnicity was collected at recruitment and grouped using the Office for National Statistics classification. Socioeconomic position was measured using the Indices of Multiple Deprivation, a nationwide deprivation rank utilising multiple datasets based on home address. Outcomes included the duration from symptom onset to first appointment in paediatric rheumatology, and change in HRQoL (measured using the Child Health Questionnaire, CHQ-50) and disease activity (measured using Juvenile Arthritis Disease Activity Score, JADAS-71) in the twelve months following initial presentation. Associations between disease duration to initial presentation, presentation and referral source with ethnicity and socioeconomic position were assessed using adjusted Cox proportional hazards models. Mean change in CHQ-50 scores and disease activity between diagnosis and after twelve months were compared between ethnic groups, and socioeconomic positions using adjusted linear regression. Multiple imputation was used to handle missing covariate and outcome data.
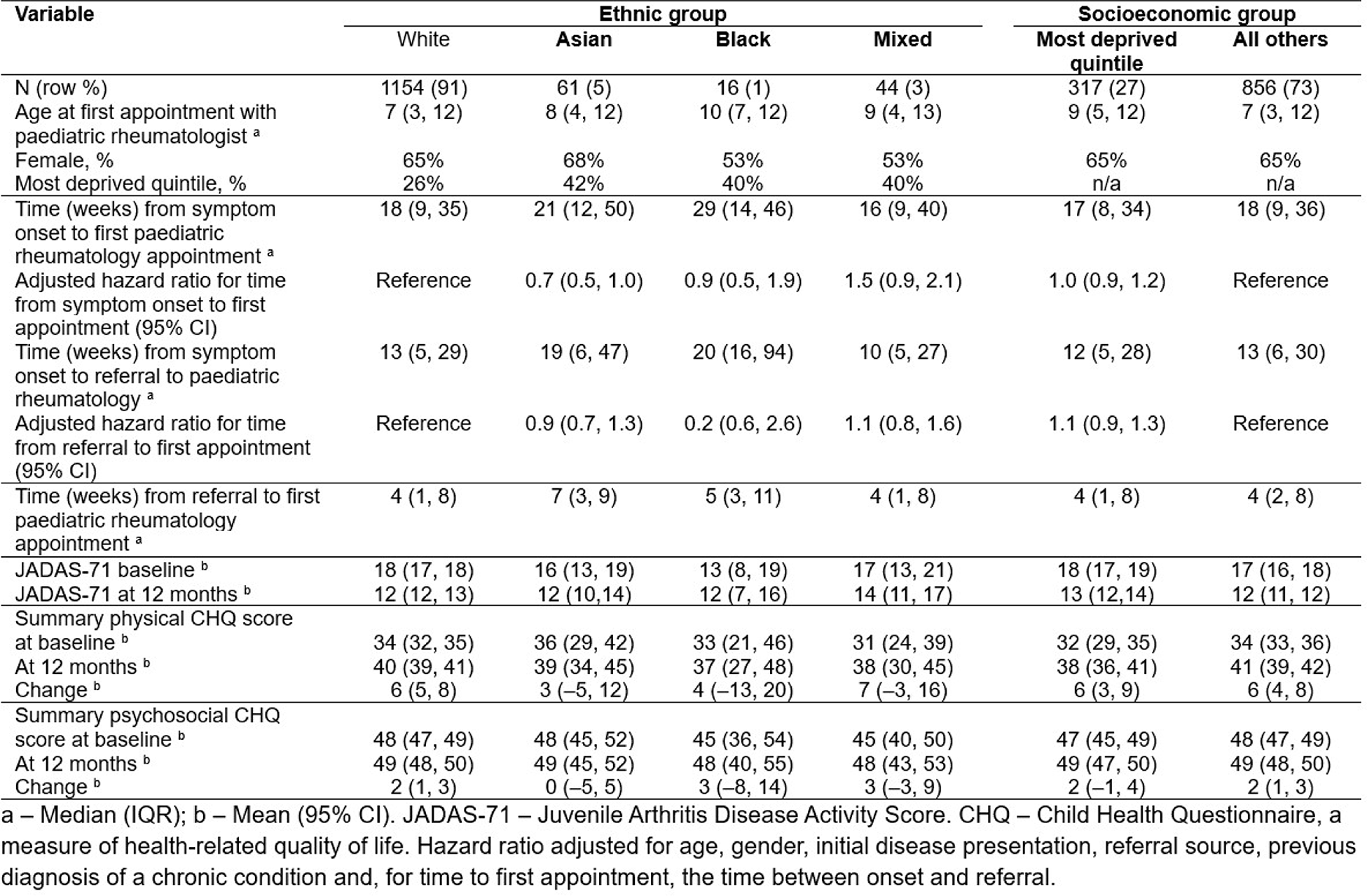
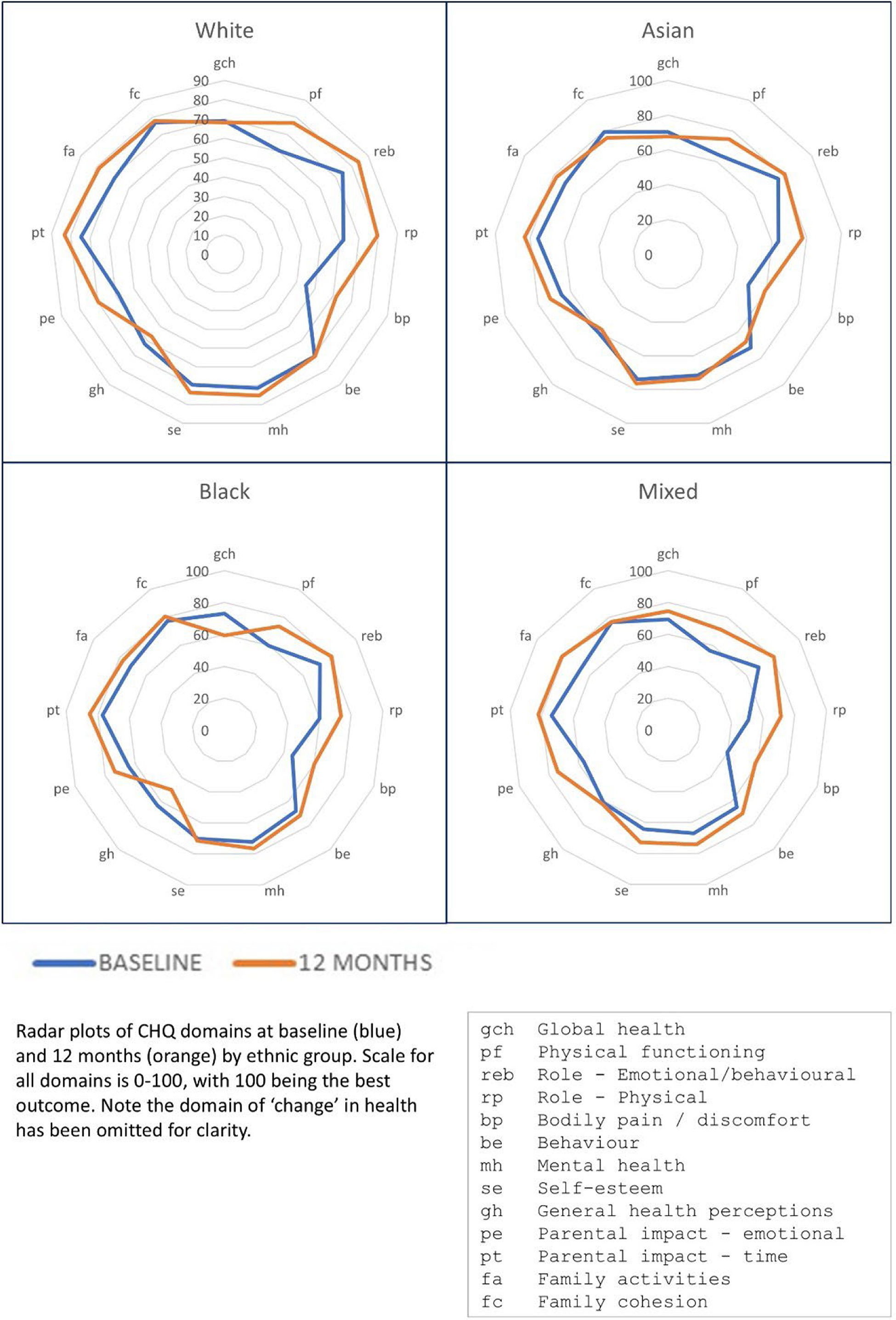
Results: A total of 1275 patients were included (median age at first appointment 8 years; 65% female). The cohort was 91% White ethnic group, 5% Asian, 1% Black, 3% Mixed, with 27% in the most deprived socioeconomic group (ranging from 26% of those of White ethnicity to 42% of those of Asian ethnicity). JIA subtypes were 49% oligoarticular onset JIA, 21% polyarticular onset, and 7% systemic JIA (Table). Median time from symptom onset to first rheumatology appointment was 18 weeks (range 16 to 29 weeks by ethnic group). There was no difference in adjusted hazard ratios for duration between symptom onset and referral to paediatric rheumatology, nor for duration from referral to paediatric rheumatology to first appointment, by ethnic group or socioeconomic group. Disease activity scores improved after twelve months across all ethnic and socioeconomic groups, and changes were not significantly associated with ethnic group or socioeconomic group. HRQoL improved across most domains and both the physical and psychosocial summary scores, with no significant differences between ethnic groups or socioeconomic groups (Figure).
Conclusions: In this UK inception cohort, overall CHQ score changes at 12 months were small across all groups, but the confidence intervals suggest meaningful variability by ethnicity and socioeconomic status. Children from Asian, Black and Mixed ethnic groups, and those from more deprived socioeconomic backgrounds, showed wider and often non-significant confidence intervals indicating greater heterogeneity in functional outcomes and potentially less consistent improvement over time. It appears that the majority of children and young people with JIA in this cohort experience improvements in measures of disease activity following initial rheumatology appointment. However, despite this, overall patient/parent-reported HRQoL measures show poor outcomes for both physical and psychosocial scores. There is proportionally low recruitment of children and young people from Asian, Black and Mixed ethnic groups, and a larger sample size from minority ethnic groups may offer further insight. This could be supported through targeting of health education strategies at communities with diverse ethnic populations to improve access to care.
Table 1. Time to referral, and health-related quality of life and disease activity at baseline and after 12 months, amongst children with JIA by ethnic group and socioeconomic group.
Radar plots of CHQ domains at baseline and 12 months, by ethnic group.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.