fetching data ... 
Background: CD19-targeted T cell engagers (TCEs) have the potential to induce B-cell depletion with potential better safety than CAR-T therapy and off-the-shelf convenience [1]. However, T cell dysfunction and exhaustion contribute to treatment failure following anti-CD19 bispecific TCE [2,3]. In this study, we developed CC312, a novel tri-specific TCE that integrates CD28 co-stimulation with CD3 and CD19 targeting. CD28 signaling in CC312 has been proved obviously with non-exhausted T cell phenotype [4].
Objectives: The potential of CC312 in treating relapsed/refractory autoimmune diseases will be explored in the clinical setting (NCT06888960).
Methods: This open-label study employs a standard 3 + 3 dose-escalation design to assess the safety and tolerability profile and to identify the maximum tolerated dose (MTD) of CC312 in an autoimmune disease population. The trial features two distinct, sequentially enrolled administration cohorts, Intravenous (IV) cohort: CC312 is administered intravenously twice per week at 5 different dose levels (5 to 40 μg). Subcutaneous (SC) cohort: CC312 is administered subcutaneously twice per week at 4 different dose levels (120 to 1440 μg). Safety, pharmacokinetic/pharmacodynamic profiles, and primary efficacy parameters—including B-lymphocyte counts of peripheral blood and bone marrow, autoantibodies and biomarkers—will be evaluated for 48 weeks. Primary efficacy endpoint is the SLE Responder Index 4 (SRI-4) criteria.
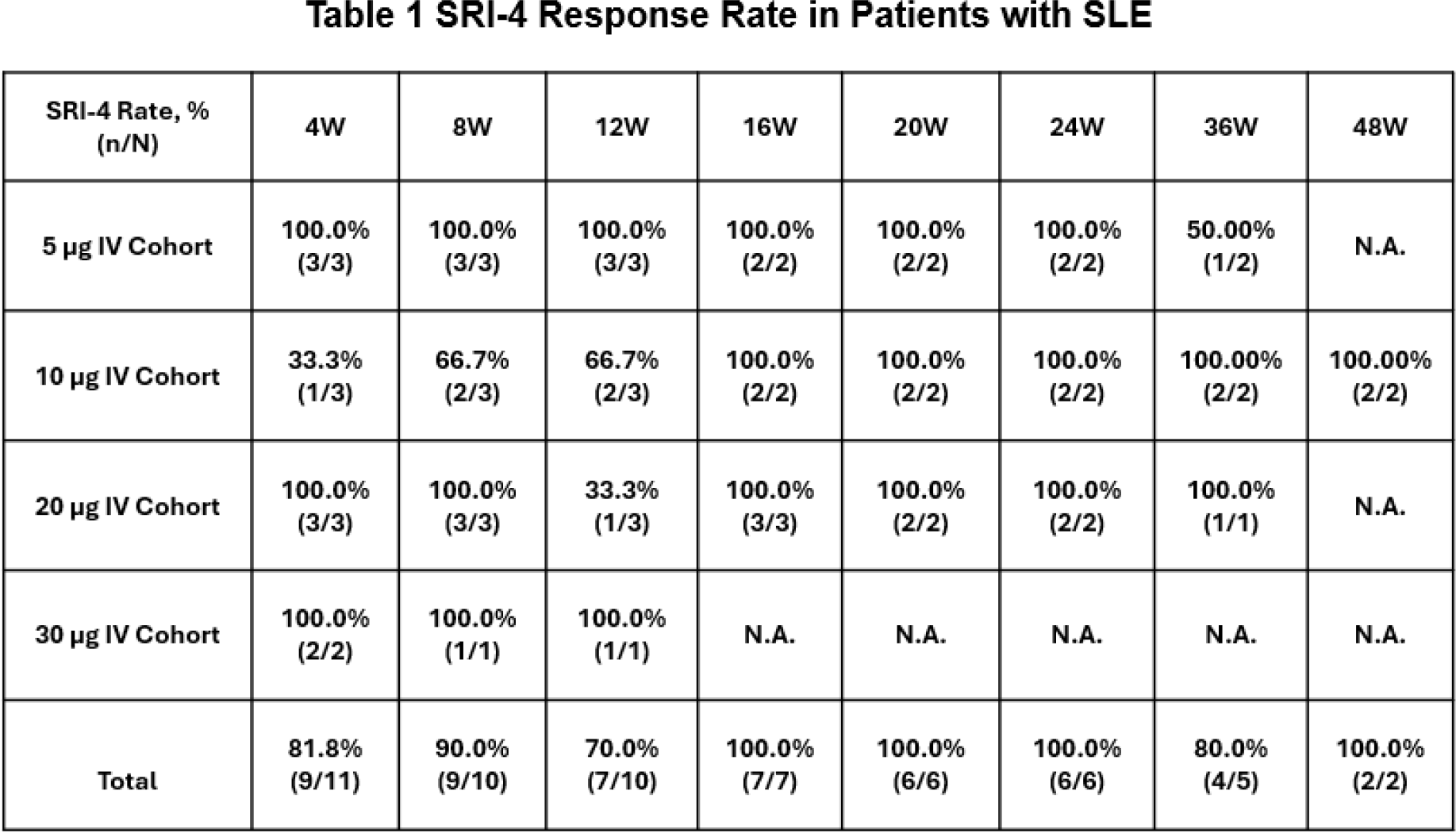
Results: To date, IV cohort: 11 patients with refractory SLE received 1 to 3 cycles of CC312 treatment. The safety profile remained favorable, with no observed dose-limiting toxicities (DLTs), immune effector cell-associated neurotoxicity syndrome (ICANS), or cytokine release syndrome (CRS) of grade ≥2. A consistent pattern of low-level release for CRS-associated cytokines (IL-6, TNF-α, and IL-10) was observed. For the current dosages, CC312 consistently and dose-dependently depleted peripheral B cells in most patients. Among those patients who were followed up ≥24 weeks, B cell reconstitution was observed at week 24 without recurrence of clinical symptoms, suggesting immune reconstitution. CD19 + B cells subsets of bone marrow were completely diminished in the cohorts (≥20 μg) at week 4 to week 12. The SRI-4 response rates are shown in Table 1. 80% of patients (4/5) achieved an SRI-4 response at week 36, with decreased SLEDAI-2K scores and improvement in clinical symptoms, 100% responders have maintained SRI-4 response. Patient 4 & 5 have maintained this response up to 48 weeks. SC cohort: This cohort has initiated the enrollment. Data collection is underway.
Conclusions: In this study, CC312 still exhibited favorable safety profiles, with no ICANS or grade ≥2 CRS at the current highest dose cohort. Rapid, near-complete depletion of peripheral CD19 + B lymphocytes was achieved at all cohorts. Furthermore, CC312 drove 100% depletion of CD19 + bone marrow plasma cells in SLE patient treated with 20 ug CC312. Long-term (up to 6~12 months) SRI-4 response was observed across the cohorts and improvement in clinical symptoms.
REFERENCES: [1] Michaelson JS, Baeuerle PA. J Exp Med. 2024;221(5): e20240499.
[2] Nora Philipp, et al. Blood. 2022 Sep 8;140(10):1104-1118.
[3] Virginie Nägele, et al. Exp Hematol Oncol. 2017 May 18:6:14.
[4] Etienne Humblin, et al. Sci Immunol. 2023 Aug 4;8(86): eadg0878.
Acknowledgments: NIL.
Disclosure of Interests: None declared.