fetching data ... 
Objectives: This study explored the relationship between clinical phenotypes and immuno-molecular features of systemic lupus erythematosus (SLE) using unsupervised machine learning and multi-omics integration.
Methods: A multicenter cohort of 1,065 SLE patients from five teaching hospitals was studied. Unsupervised clustering was performed using integrated clinical and laboratory data to identify distinct phenotypic clusters. Multi-omics profiling, including proteomics and transcriptomics, was conducted for each cluster, comparing with healthy controls. In addition, 899 patients were prospectively followed for over one year to assess therapeutic responses and remission outcomes.
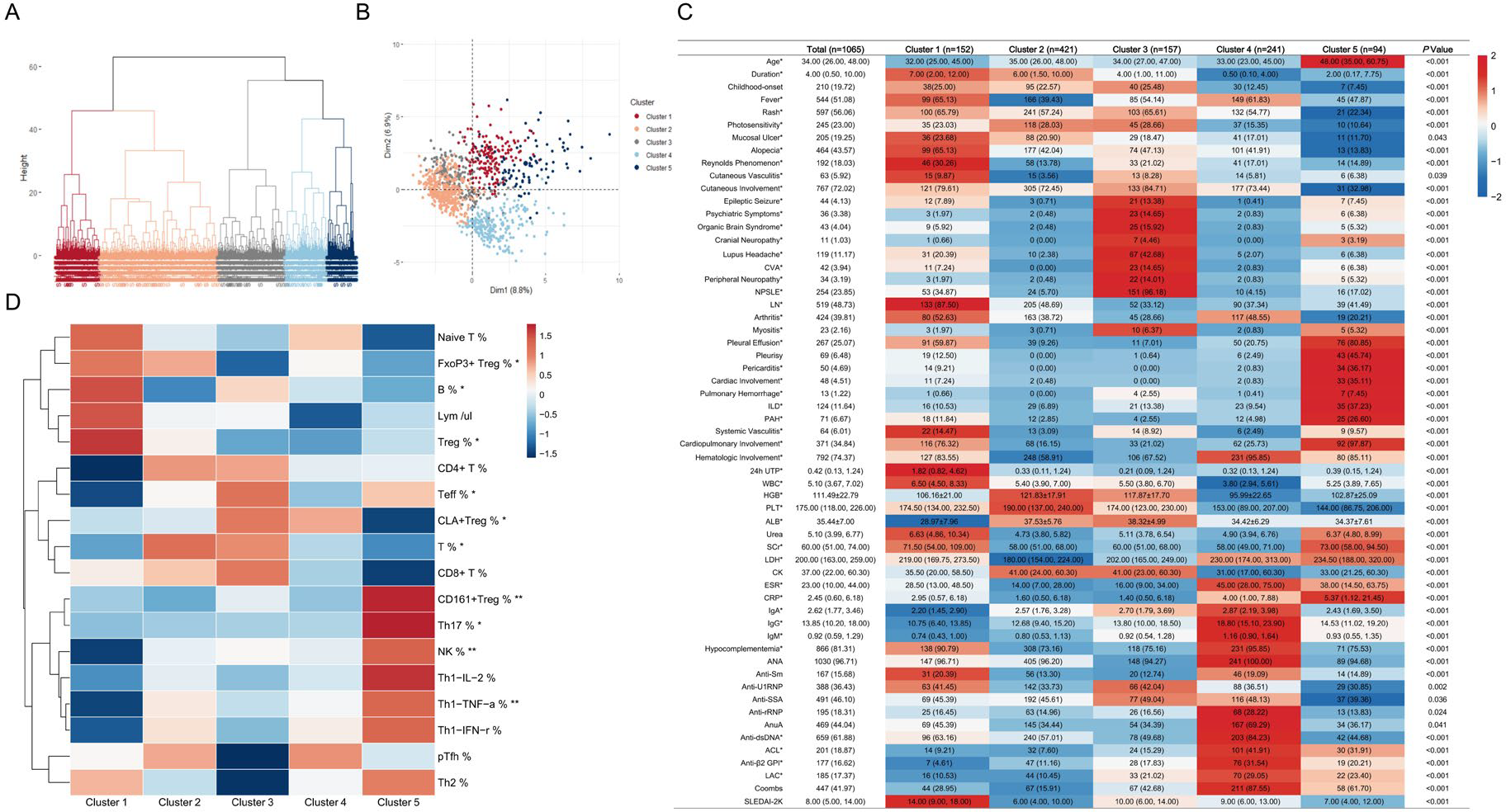
Results: Unsupervised clustering identified five distinct clusters of SLE based on clinical phenotypes and immunological signatures, and an intrinsic association was found between each cluster and immune-inflammatory features. Cluster 1 (renal; 14.27%) had predominant renal involvement (87.5%) and high disease activity. Cluster 2 (mucocutaneous; 39.53%) exhibited mainly cutaneous manifestations (72.45%) with mild visceral involvement and the highest rates of achieving low disease activity state (46.42%). Cluster 3 (neuropsychiatric; 14.74%) had a high frequency of neuropsychiatric manifestations (96.18%) and anti-U1RNP antibody positivity (42.04%). Cluster 4 (hematologic; 22.63%) was characterized by hematologic involvement, predominantly cytopenia (95.85%), with frequent antiphospholipid antibody positivity and direct Coombs positivity (87.55%). Cluster 5 (cardiopulmonary; 8.83%) exhibited prominent cardiopulmonary involvement (97.87%) and serositis, with enrichment of inflammatory CD161 + regulatory T cells. Transcriptomic and proteomic analyses confirmed distinct molecular signatures and cluster-specific enrichment of biological pathways. Key molecule apolipoprotein A4 was validated using ELISA. Regarding therapeutic outcomes at one-year follow-up, Cluster 2 had the highest proportions achieving lupus low disease activity state (46.42%) and tapering glucocorticoids. Cyclophosphamide use was associated with greater clinical improvement (r = 0.284; P = 0.023) in Cluster 3, while in Cluster 5, rituximab use was associated with favorable responses (r = 0.286; P = 0.019).
Conclusions: We identified five SLE clusters with distinct clinical, immunological features and treatment outcomes, demonstrating an intrinsic link between clinical involvement and immune-inflammatory alterations.
Integrated Characterization of Clinical and Immunologic Heterogeneity in Systemic Lupus Erythematosus. (A) Identification of five distinct patient clusters through hierarchical clustering analysis. (B) Factor map visualization of patient distribution colored by corresponding cluster affiliation. (C) Heatmap displaying clinical and serological characteristics across the five clusters. Color intensity represents z-score standardized differences relative to other patients. Variables marked with asterisks were included in the clustering analysis. Continuous variables are presented as mean ± standard deviation for normally distributed data and as median (interquartile range [IQR]) for non-normally distributed data; categorical variables are shown as number (percentage). (D) Distribution patterns of peripheral blood lymphocyte subsets (z-score normalized) across clusters, with red indicating enrichment and blue indicating depletion. Statistical significance is denoted as follows: *P < 0.05, **P < 0.01, ***P < 0.001.
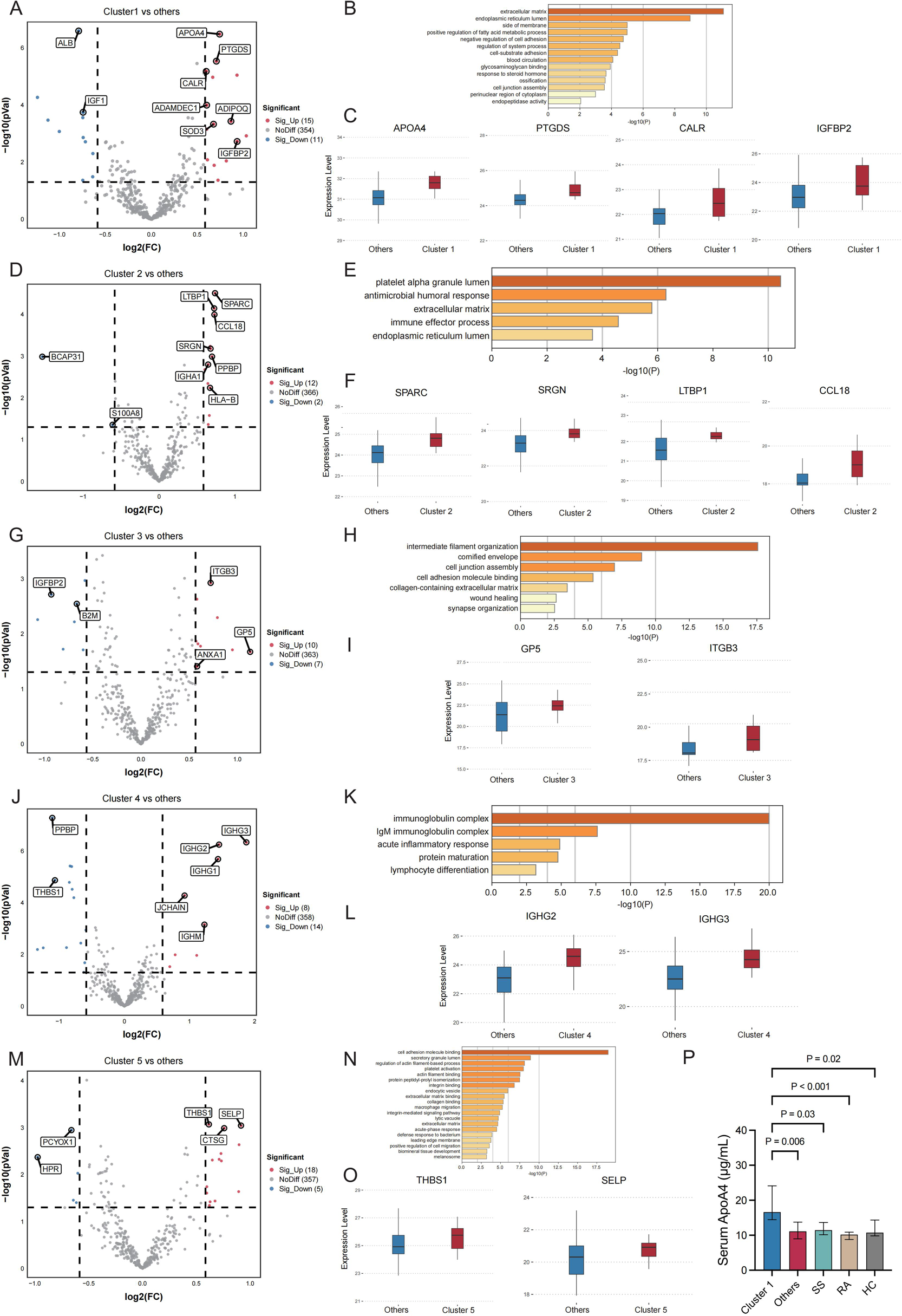
Differential Proteomic Profiling Between SLE clusters. Volcano plots (A, D, G, J, M) display differentially expressed proteins in Cluster 1-5 versus the other four clusters, respectively; (C, F, I, L, O) illustrate upregulation of key proteins in SLE 1-5; Enrichment analysis plots (B, E, H, K, N) illustrate functional pathways of differentially expressed proteins specific to Cluster 1-5 Violin plots. Serum apolipoprotein A4 (APOA4) levels were validated by ELISA and were significantly higher in Cluster 1 than in other SLE clusters, primary Sjögren’s syndrome (SS), rheumatoid arthritis (RA), and healthy controls (HC) (P).
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.