fetching data ... 
Background: Systemic sclerosis (SSc) is a complex systemic autoimmune rheumatic disease that presents with inflammatory and fibrotic changes involving the skin, lungs, gastrointestinal tract, and blood vessels. SSc can be diagnosed at any age, but most commonly around 30-50 years of age. The aim of this study is to improve our understanding of the epidemiology of geriatric SSc. This study provides a detailed comparative analysis of people diagnosed with SSc at age 65 or older (Late-onset Systemic Sclerosis, LoSSc ) and those diagnosed before 65 years (Early-onset Systemic Sclerosis, EoSSc ). Understanding these differences is important for developing optimized care for our senior adult population.
Objectives: The objectives of this study are to compare the demographic characteristics, SSc-specific clinical manifestations, comorbidity burden, survival outcomes, and predictors of mortality in people with LoSSc and EoSSc.
Methods: We conducted a cohort study of the Toronto Scleroderma Program. Patients were included if they fulfilled the ACR/EULAR classification criteria for SSc. The primary outcome was the time from diagnosis to death from all causes. Secondary outcomes included differences in calcinosis, Raynaud phenomenon, digital ulceration, esophageal dysmotility, telangiectasia, interstitial lung disease (ILD), pulmonary arterial hypertension (PAH), scleroderma renal crisis, NYHA functional class, and serology. Comorbidities were evaluated individually and cumulatively as a measure of the burden of multi-morbidity. Descriptive statistics, relative risk (RR) with 95% confidence intervals (CI) were used to compare patients. Kaplan Meier curves and Cox models were used to evaluate survival.
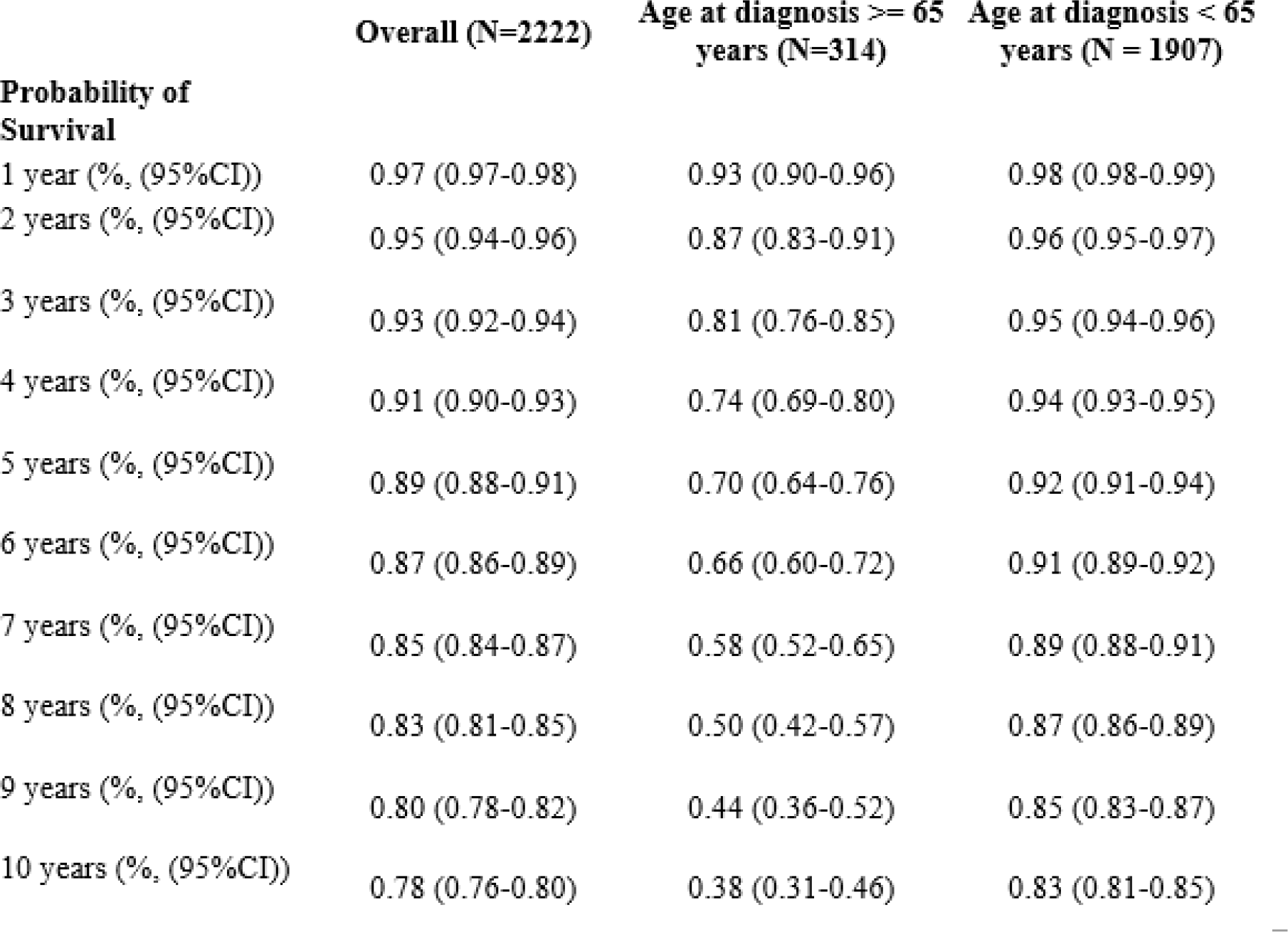
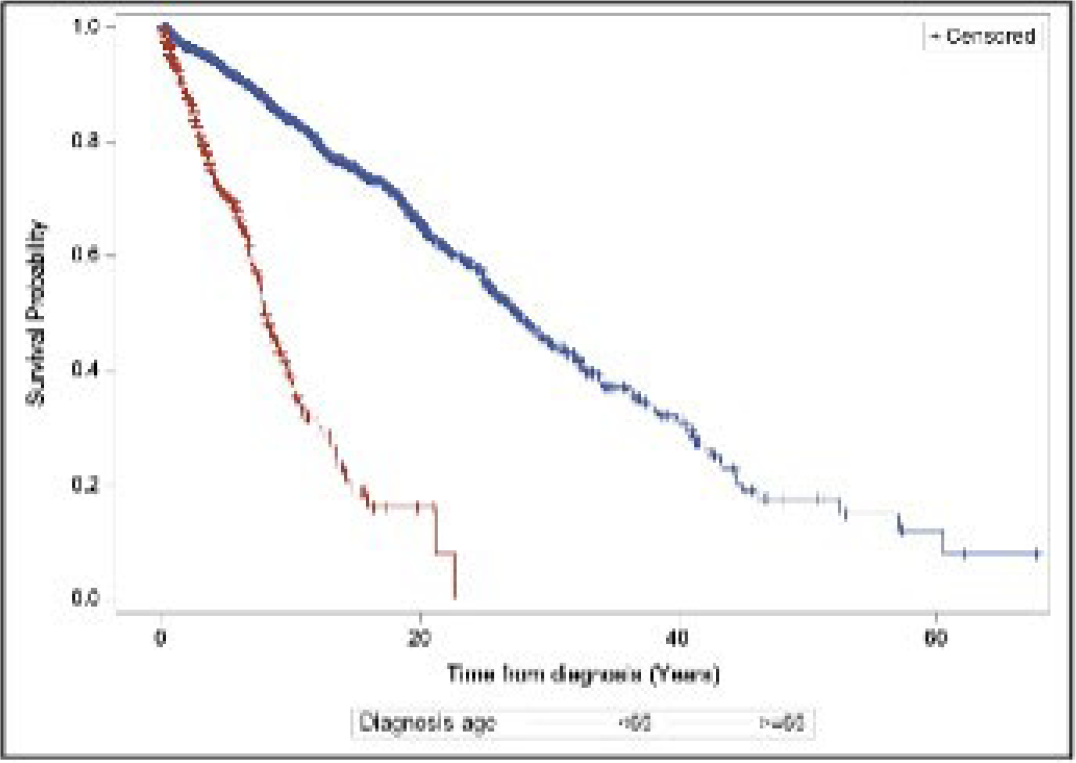
Results: 2303 SSc patients were included, with 1976 EoSSc and 327 LoSSc . LoSSc patients were significantly less likely to have esophageal dysmotility (RR 0.91, 95% CI 0.85-0.97), digital ulcers (RR 0.65, 95% CI 0.53-0.81), and anti-Scl-70 antibodies (RR 0.68, 95% CI 0.51-0.91). LoSSc patients were significantly more likely to have pulmonary arterial hypertension (RR 1.59, 95% CI 1.33-1.89), coronary artery disease (RR 2.72, 95% CI 2.08-3.57), systemic hypertension (RR 2.22, 95% CI 1.92-2.56), diabetes mellitus (RR 1.98, 95% CI 1.41-2.78), hyperlipidemia (RR 2.31, 95% CI 1.80-2.95), peripheral vascular disease (RR 2.36, 95% CI 1.39-4.03), cancer (RR 2.34, 95% CI 1.85-2.96), stroke (RR 1.92 (95% CI 1.04-3.54), and atrial fibrillation (RR 4.19, 95% (3.00-5.85). They were also more likely to be NYHA functional class II or higher (RR 1.50, 95% CI 1.17-1.92). LoSSc patients have a significantly higher burden of multimorbidity, with a risk of 6 or more comorbidities of RR 26.9 (95% CI 2.46-293) LoSSc patients had significantly higher mortality at 1-year, 5-years and 10-years. Table 1, Figure 1. On univariate analysis, LoSSc was an independent predictor of mortality (Hazard ratio (HR) 5.02 p<0.0001) and remained an independent risk factor for mortality (HR 4.51, p<0.0001) after adjusting for male sex, diabetes, hypertension, stroke, ILD, pulmonary arterial hypertension, renal crisis and cancer.
Conclusions: People with LoSSc exhibit a higher burden of comorbidities, increased prevalence of pulmonary arterial hypertension, and poorer survival rates compared to their EOSSc. These findings underscore the importance of tailored screening, monitoring, and prognostic counselling for geriatric SSc patients and their families.
Table 1. Comparison of probability of short and long term survival.
Kaplan Meier survival curves comparing people with SSc diagnosed at age 65 or older (Late-onset Systemic Sclerosis, LoSSc ) and those diagnosed before 65 years (Early-onset Systemic Sclerosis, EoSSc ).
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.