fetching data ... 
Background: Anti-CD19 chimeric antigen receptor T-cells (CART) have demonstrated sustained remissions in active systemic lupus erythematosus (SLE) through deep depletion of pathogenic B-cells and pan-immune “reset” of pathogenic inflammatory cascades[1,2,3,4]. CD3xCD19 Bi-specific T-cell engagers (TCE) are capable of similar B cell depletion, with more convenient dosing and without the need for pre-treatment lymphodepletion[5,6,7]. A-319 is a novel TCE targeting CD3 and CD19, that has demonstrated favorable tolerability and efficacy in prior studies of patients with B-cell tumors [8]. We hypothesized that A-319 could be utilized in SLE to achieve depletion of autoreactive B-cells, thereby resetting pathogenic autoimmune circuits [9]. Here, we present efficacy and safety data for A-319, a potent CD3×CD19 TCE, in 12 patients with active SLE.
Objectives: The primary study endpoint was safety and tolerability of A-319 in patients with active SLE. Adverse events (AEs) and dose-limiting toxicity (DLT) were collected and included in safety analyses for all participants from the first dose of study drug until study withdrawal or completion of the study. Secondary endpoints included pharmacokinetic (PK) and pharmacodynamic (PD) characterization of A-319, and exploratory endpoints included assessment of peripheral B-cell depletion, clinical efficacy, and effect on peripheral blood mononuclear cell (PBMC) gene expression.
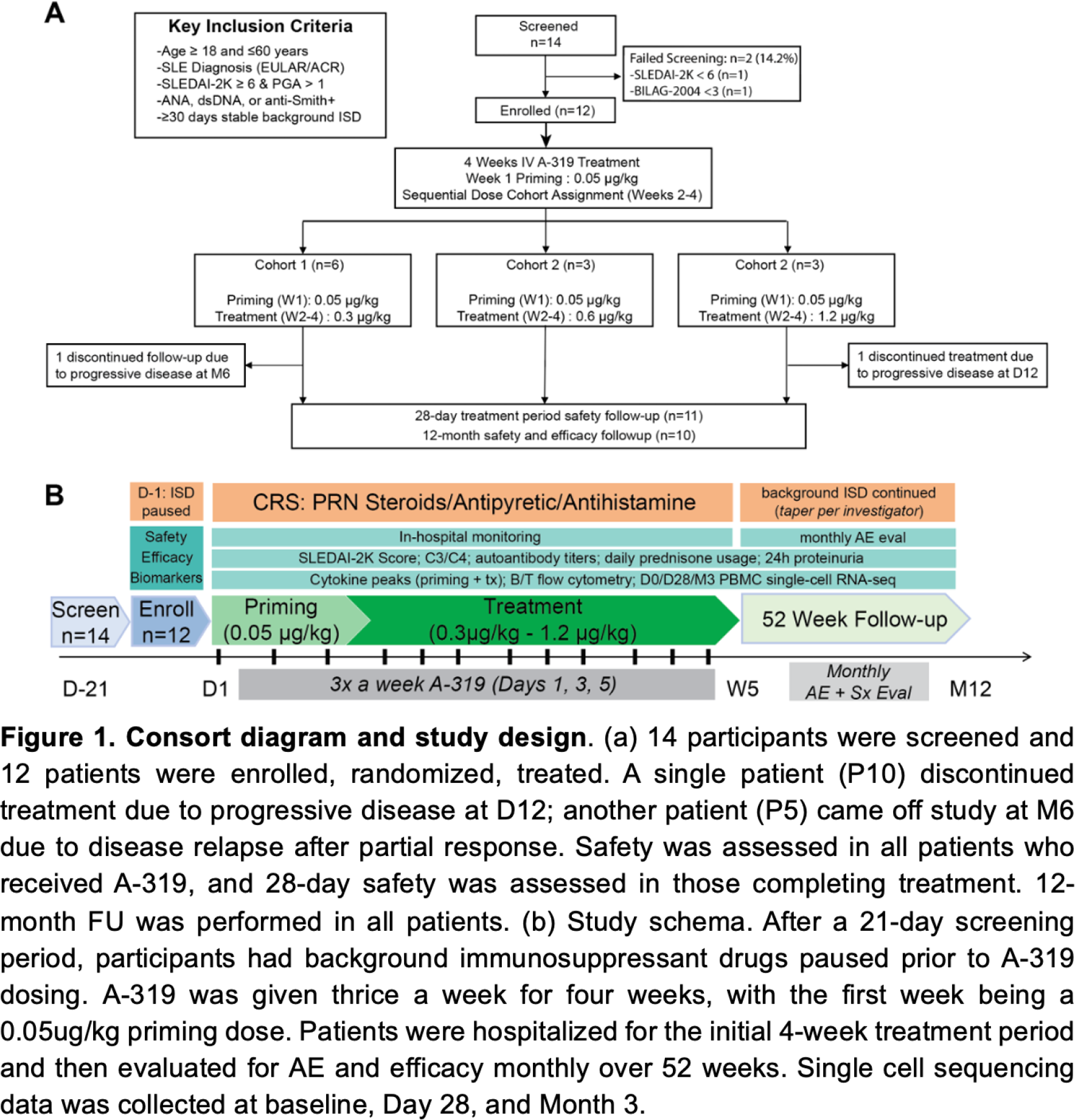
Methods: This investigator-initiated, open-label dose escalation study was conducted at 2 centers in China (NCT06400537). The study consisted of a 3-week screening period, a 4-week treatment period, and a 12-month follow-up period ( Figure 1a ). After receiving three priming doses of 0.05 μg/kg, patients were sequentially enrolled to three A-319 doses: 0.3 μg/kg (n=6), 0.6 μg/kg (n=3), and 1.2 μg/kg (n=3, Figure 1b ). All doses were administered intravenously (IV). Eligible participants were 18 to 60 years of age with a clinical diagnosis of SLE for ≥ 24 weeks according to the 2019 American College of Rheumatology and the European League Against Rheumatism (EULAR) classification criteria 10 . Active SLE was defined by Systemic Lupus Erythematosus Disease Activity Index 2000 11 (SLEDAI-2K) score ≥6, Physician Global Assessment 12 (PGA score) > 1, with ≥1 organ system meeting British Isles Lupus Assessment Group 2004 Index 13 (BILAG-2004) A or ≥2 organ systems meeting BILAG-2004 B criteria. Efficacy analyses were conducted in the full analysis population. Safety analyses involved all the participants who had received at least one dose of A-319. SLE clinical response was assessed by the SLEDAI-2K, PGA, BILAG-2004, SLE Responder Index (SRI)-4, 6, 8, Lupus Low Disease Activity State (LLDAS) criteria 14 , and Definition of Remission in SLE 15 (DORIS) at every visit from Week 4 to Week 52. Molecular biomarkers, including autoantibody titers, complement levels, 24-hour urinary protein excretion, urine protein creatinine ratio (UPCR), and peripheral B-cell count were assessed at each follow-up visit. Peripheral blood mononuclear cell (PBMC) gene expression was measured using serial single-cell sequencing (10X Genomics) at baseline (Day 0), intra-treatment (Day 28), and post-treatment (Month 3) and analyzed using custom genomic pipelines in R v4.0.5 16 .
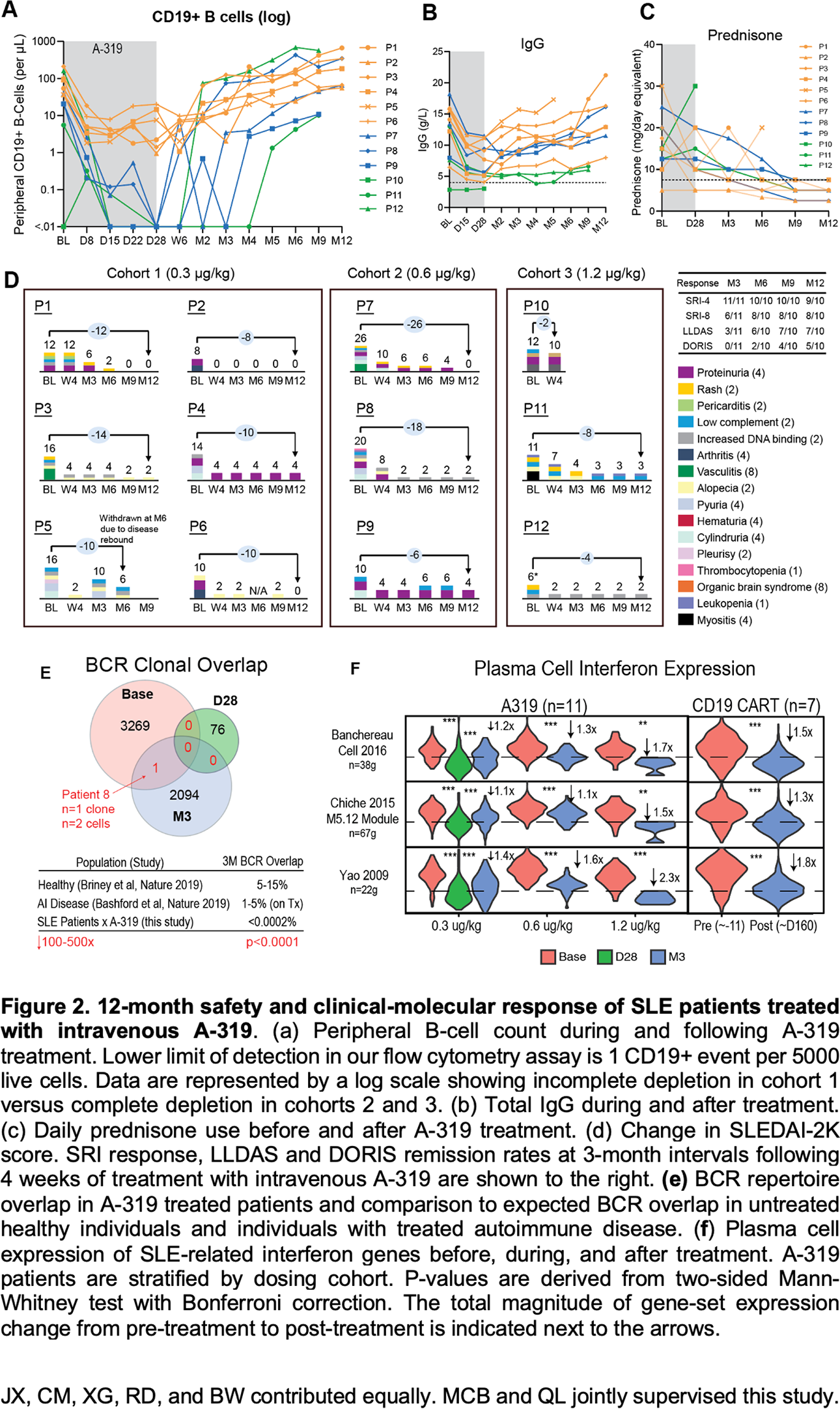
Results: From July 2024 through January 2025, 12 patients with SLE were enrolled and treated with A-319. All patients were female, with a mean age of 35.9 years (range: 21-54), mean disease duration of 9.1 years (range 0.5-26), and mean SLEDAI-2K score of 14.1 (range: 6-26). All patients failed two or more lines of standard therapy, and 8 patients had failed prior biologic therapy. A319 was well tolerated. 11 of 12 enrolled patients completed the 4-week treatment period. One patient (P10) experienced elevated inflammatory markers, serositis and worsened proteinuria, resulting in withdrawal from the study at Day 12. Grade 1 cytokine release syndrome (CRS) occurred in 10 patients, and Grade 2 CRS occurred in one patient. All instances of CRS resolved within 12 hours with supportive care. No instances of immune effector cell-associated neurotoxicity syndrome (ICANS) were observed. B-cell nadir occurred by week 4 in all patients. Patients in cohorts 2 (0.6ug/kg) and 3 (1.2ug/kg) experienced complete B-cell depletion, while patients in cohort 1 (0.3ug/kg) experienced incomplete B-cell depletion (mean: 90% depletion, Figure 2b ). The duration of B-cell aplasia was dose-dependent (mean: 1.5 months; range: 0-6). 1 patient experienced hypogammaglobulinemia (IgG <4 g/L) requiring IVIG ( Figure 2b ), 2 patients experienced neutropenia (grade 1), and 1 patient experienced thrombocytopenia (grade 1). 11 patients had meaningful reductions in the SLEDAI-2K after treatment. At 12-month follow-up, we observed a 69% reduction in daily steroid use (mean: 16.9mg to 5.25mg), with 10 patients achieving LLDAS-7.5 response (Figure 2c ) and 5 patients achieving DORIS remission ( Figure 2d ). In 4/6 patients with baseline 24h urinary protein ≥ 500mg, we observed normalization of 24h urinary protein (< 500mg). Serial kidney biopsies from two of these patients showed CD19 depletion, markedly reduced immune complex deposition and reduction in NIH Lupus Nephritis activity indices post-treatment. Serial single-cell RNA-sequencing of PBMCs and comparison to CD19 CART data 4 revealed analogous reduction in inflammatory signaling in T, B, and myeloid subsets, elimination of pathogenic memory B-cells, and dose-dependent “reset” of interferon-high plasma-cells ( Figure 2e-f ).
Conclusions: A-319 demonstrates a favorable safety profile in patients with treatment refractory SLE. Treatment with A-319 resulted in rapid B-cell depletion and sustained molecular and clinical responses. Integrated analysis of serial scRNA-sequencing data from A-319 and CD19-CART treated patients indicate analogous “reset” of pathologic gene expression in lymphoid and myeloid immune populations, and a “reset” of the B-cell repertoire, supporting further clinical development of A-319 in active SLE.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Jason Xu: None declared, Chunli Mei: None declared, Xin Guan: None declared, Rong Du: None declared, Bin Wu: None declared, Di Wu: None declared, Mengjiao Li: None declared, Jingna Li: None declared, You Song: None declared, Xiaoqi Chen: None declared, Tamiko R. Katsumoto TRK received research funding from Sanofi, Xiaoqiang Yan XQ holds shares in iTabMed Ltd., Eric Meffre: None declared, Jonathan Sussman: None declared, Qianyu Guo: None declared, Hanyang Chen is an employee of iTabMed Ltd, Vanessa Kennedy: None declared, Anbing Huang: None declared, Matthew Baker MCB consults for Sanofi, AbbVie, Neurocrine, Qiubai Li: None declared.