fetching data ... 
Background: Antinuclear antibody (ANA) is a pivotal diagnostic indicator in rheumatic and musculoskeletal diseases (RMDs) but has low specificity [1]. Hence, ANA-positive people with non-specific symptoms are an at-risk population for several ANA-associated RMDs. Interferon (IFN)-stimulated gene expression scores, which have experienced a rapid escalation in research focus, might predict progression from ANA positivity to RMDs [2]. Tetherin (also known as CD317 or BST-2), is an IFN-I inducible cell surface protein encoded by BST2 gene and expressed on all nucleated cells, providing a cell-specific biomarker of IFN pathway activation useful to compare IFN-I response across circulating subsets [3].
Objectives: (i) To validate IFN scores as biomarkers of imminent RMDs. (ii) To analyse a wider range of transcriptomic modules and a cell-specific flow cytometric IFN marker (tetherin) longitudinally to investigate pathogenesis.
Methods: 181 individuals including 5 healthy controls and 176 patients with ANA and new non-specific symptoms were recruited. Progression to RMDs was defined as diagnosis of systemic lupus erythematosus (SLE) (2019 EULAR/ACR classification criteria), systemic sclerosis (SSc) (2013 ACR/EULAR classification criteria), primary Sjögren’s syndrome (pSS) (2016 ACR/EULAR classification criteria), or idiopathic inflammatory myopathies (2017 EULAR/ACR classification criteria) during the 12-month follow-up period. Peripheral blood mononuclear cells (PBMCs) were isolated for RNA extraction and flow cytometric analysis. Expression of previously validated transcriptomic scores known to be associated with RMDs (IFN Score A, IFN Score B, Plasmablast, Myeloid, Inflammation and Erythropoiesis Scores) were calculated using a 96-gene TaqMan array [4,5]. Cellular abundance and median fluorescence intensity (MFI) of tetherin were measured by flow cytometric gating for B cells, memory B cells, plasmablasts, T cells and. Different monocyte subsets of tetherin MFI were further analysed. We compared the odds ratios for progression to RMDs utilizing multivariable logistic regression model.
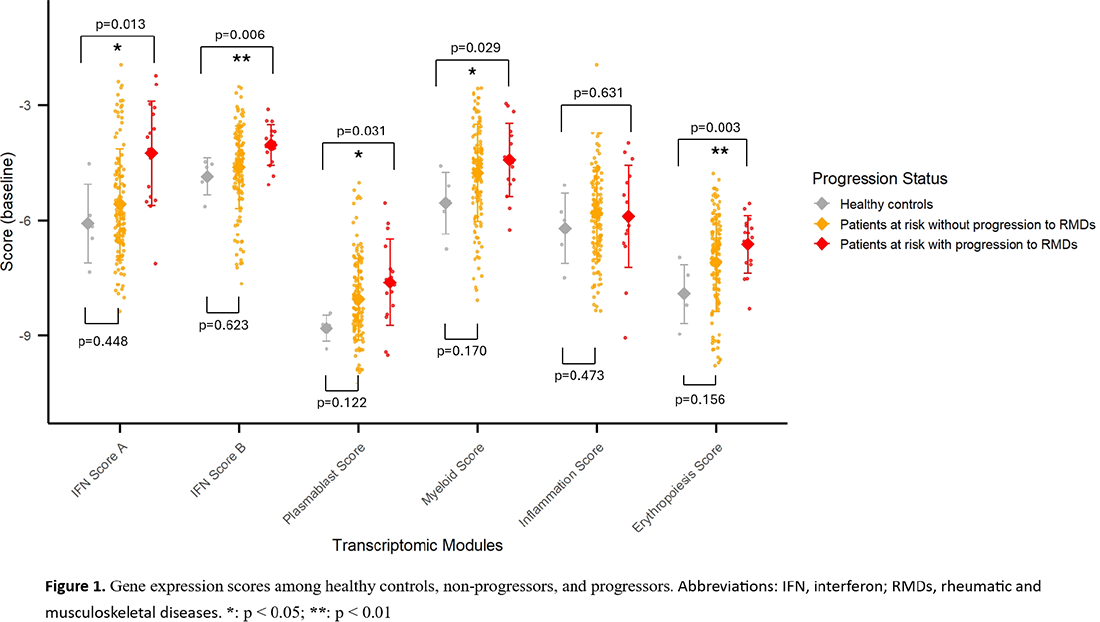
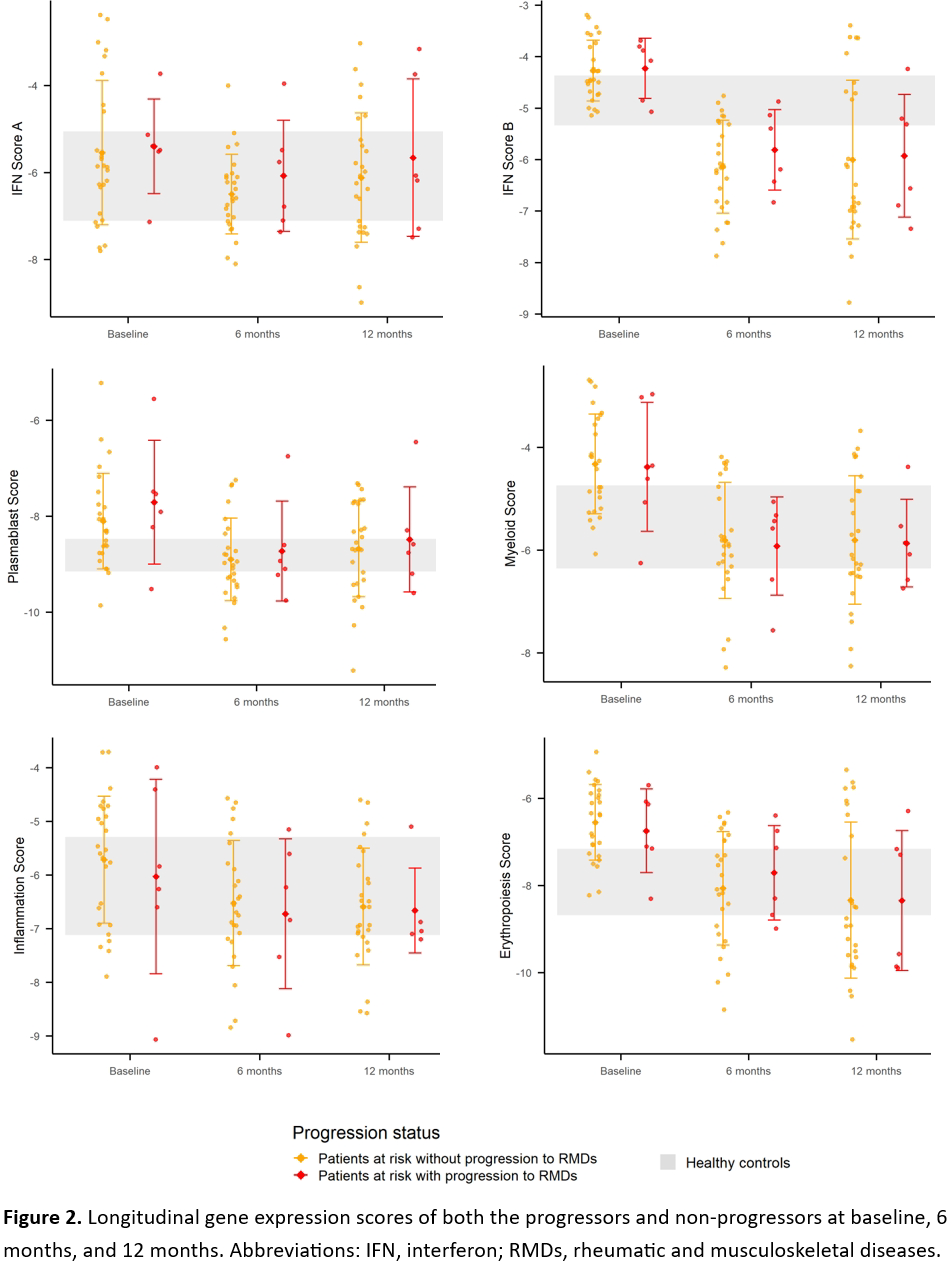
Results: Progression occurred in 17/176 (9.7%) patients (11 SLE, 4 pSS, 1 SSc, and 1 SLE-SSc overlap). Most clinical and demographic variables including age, gender, ethnicity, family history of RMDs, smoking status, neutrophil and monocyte counts did not differ between progressors and non-progressors at baseline, although the proportion of Caucasian was slightly lower in progressors (progressors versus non-progressors: 64.7% versus 75.5%, respectively; Fisher’s exact test p-value=0.382; effect size=0.24). Leukocyte and lymphocyte counts at baseline were significantly lower among progressors (progressors versus non-progressors: 5.43±1.15 versus 6.56±1.89 10 9 /L in leukocyte count with p-value=0.001, 1.48±0.37 versus 1.88±0.65 10 9 /L in lymphocyte count with p-value<0.001, respectively). Comparing the gene expression scores of both progressors and non-progressors at baseline with those of healthy controls, progressors had significantly higher IFN Score A, IFN Score B, Plasmablast, Myeloid and Erythropoiesis Scores, while no significant differences were observed in any of scores in non-progressors ( Figure 1 ). In multivariable logistic regression model adjusting by age, gender, ethnicity, lymphocyte count, and monocyte count, IFN Score A at baseline (OR=1.493, 95% CI=1.015-2.195, p-value=0.042), IFN Score B at baseline (OR=2.080, 95% CI=1.015-4.262, p-value=0.046), and the proportion of B cells in PBMC at 12 months (OR=1.139, 95% CI=1.002-1.295, p-value=0.046) were significantly associated with progression to RMDs. Analysing cell-specific IFN pathway activation in multivariable logistic regression, tetherin MFI (divided by 10 4 ) in T cells at 6 months was significantly associated with progression to RMDs (OR=4.194, 95% CI=1.378-12.766, p-value=0.012), and with a similar trend in B cells at baseline (OR=3.283, 95% CI=0.977-11.029, p-value=0.055). Surprisingly, we observed reduction in most gene expression scores over time in both progressors and non-progressors ( Figure 2 ). Further analysis revealed that regardless of medication status (hydroxychloroquine or immunosuppressants), both the treatment and non-treatment groups exhibited a consistent decline in all scores across the study period. Among progressors, there were similar downward trends in tetherin expression in most immune cell subsets except for monocytes, which showed an increase over time. Focusing on change of tetherin expression in different subsets of monocytes, we found that the increase in tetherin MFI was limited to nonclassical monocytes (52193.8±16162.7, 57931.5±16006.0, and 60595.7±10008.2 at baseline, 6 months, and 12 months, respectively), and was not observed in classical monocytes.
Conclusions: Both IFN Score A and IFN Score B were validated as independent predictors of progression to RMDs. Although other gene expression signatures known to be associated with RMDs did not exhibit a decisive role in disease initiation, most at baseline among progressors showed significant increases compared with those among healthy controls. Flow cytometric analysis suggests that IFN-pathway activation in B cells and nonclassical monocytes differentiation is an appropriate set of targets for prevention therapy in high-risk individuals. The reduction in transcriptomic profiles over time might represent onset of the immune exhaustion.
REFERENCES: [1] Bossuyt, X., et al. Nat Rev Rheumatol, 2020. 16(12): p.715–726.
[2] Md Yusof, M.Y., et al. Annals of the Rheumatic Diseases, 2018. 77(10): p.1432–1439.
[3] El-Sherbiny, Y.M., et al. Arthritis Rheumatol, 2020. 72(5): p.769–779.
[4] Carter, L.M., et al. Br J Dermatol, 2023. 189(2): p.210–218.
[5] Carter, L.M., et al. Arthritis Rheumatol, 2023. 75(5): p.697–710.
Acknowledgments: NIL.
Disclosure of Interests: Han-Hua Yu: None declared, Jack Arnold Alumis and UCB, Zoe Wigston: None declared, Lucy M. Carter Alumis Inc, UCB Biopharma SRL, Otsuka Pharmaceuticals UK Ltd (Unrestricted educational grant paid to employer), Md Yuzaiful Md Yusof Speaker fees: Alumis, CSL Vifor, Novartis, Roche, and UCB, Consulting fees: Aurinia Pharmaceuticals, UCB, and Autolus. Advisory Board: GSK and Novartis, Edward M. Vital Consultancy and speaker fees: Abbvie, Alpine, Alumis, Amgen, Artiva, Aurinia, AstraZeneca, Becton Dickinson, Bedrock, Biogen, BMS, Boxer, Cabaletta, Candid, Capella, CESAS, Dianthus, Genentech, Giilead, Glenmark, GSK, ICON, Idorsia, ILTOO, Kymera, Lilly, Limbic, Medixci, Medscape, Merck, Modus, Novartis, Otsuka, Pfizer, Priovant, Rednucleus, Roche, Sandoz, Springer, System Analytic, UCB, Viatris, Ventus, Zenas,., Research Grants: Roche, Novartis, AstraZeneca.