fetching data ... 
Background: Decades of clinical research in rheumatology have shown that patients with a disadvantaged socio-economic status (SES) are more likely to have a more severe course of disease, experience a higher disease burden, and accumulate comorbidities. Health literacy (HL) had been identified as a potential link between disadvantaged SES and poor health outcomes [1-3]. HL is a multidimensional construct and determines a person’s ability of self-care and master their own health, to interact effectively with healthcare providers (HCP) and to access and utilize healthcare services [2]. In contrast to SES, HL is potentially modifiable. However, evidence is lacking on HL as a mediator between SES and health outcome and on the role of behavioural traits such as mastery in this pathway.
Objectives: The primary objective was to examine in persons with rheumatoid arthritis (RA), Spondyloarthritis (SpA) and gout whether HL mediates the relationship between SES and three different health outcomes (patient global assessment of health (PtG health), global impact of RMD on health as reported by the HCP (HCP’s impact on health) and number of comorbidities). The secondary objective was to explore whether mastery, either in a sequence with HL or alone further clarifies the relationship between SES and health outcomes.
Methods: Data were used from a multicentre study in the Netherlands, which aimed to uncover health literacy profiles among persons diagnosed with RA, SpA, and gout. Centers represented socio-economically diverse regions in the Netherlands and were requested to include a similar number of persons with each diagnosis. Information on patients’ SES included age, gender, education, work status, migration background, and living situation. Outcomes included the PtG health (visual analogue scale (VAS); 0-10=best), the HCP’s impact on health (VAS; 0-10=worst) and the count of comorbidities. HL was measured using the Health Literacy Questionnaire (HLQ), which assesses HL strengths and weaknesses across 9 domains (score 0-4 or 0-5; higher being stronger). Mastery was measured using the Pearlin Mastery Scale, which captures an individual’s sense of personal control over life events (7 items on a 4-point Likert: score 7-28=best). First, confirmatory factor analysis (CFA) was applied to ensure that the observed indicators for SES and HL reliably represent the underlying (latent) constructs. With valid measurement models of these key variables of interests established, mediation analysis was carried out within the structural equation modelling (SEM) framework, which utilised latent variables to reflect the concepts of SES and HL. Three mediation models were estimated following the same analytic structure: (1) SES → health literacy → outcomes, (2) SES → mastery → outcomes, and (3) SES → health literacy → mastery → outcomes. Indirect, direct, and total effects were extracted for each outcome. Model fit was assessed by the comparative Fit Index (CFI), Tucker-Lewis Index (TLI) (acceptable if ≥0.90 and good if≥ 0.95), Root Mean Square Error of Approximation (RMSEA) (good if <0.08) and Standardized Root Mean Square Residuals (SRMR) (good if <0.08). All models were estimated using the Lavan package in R version 4.4.0.
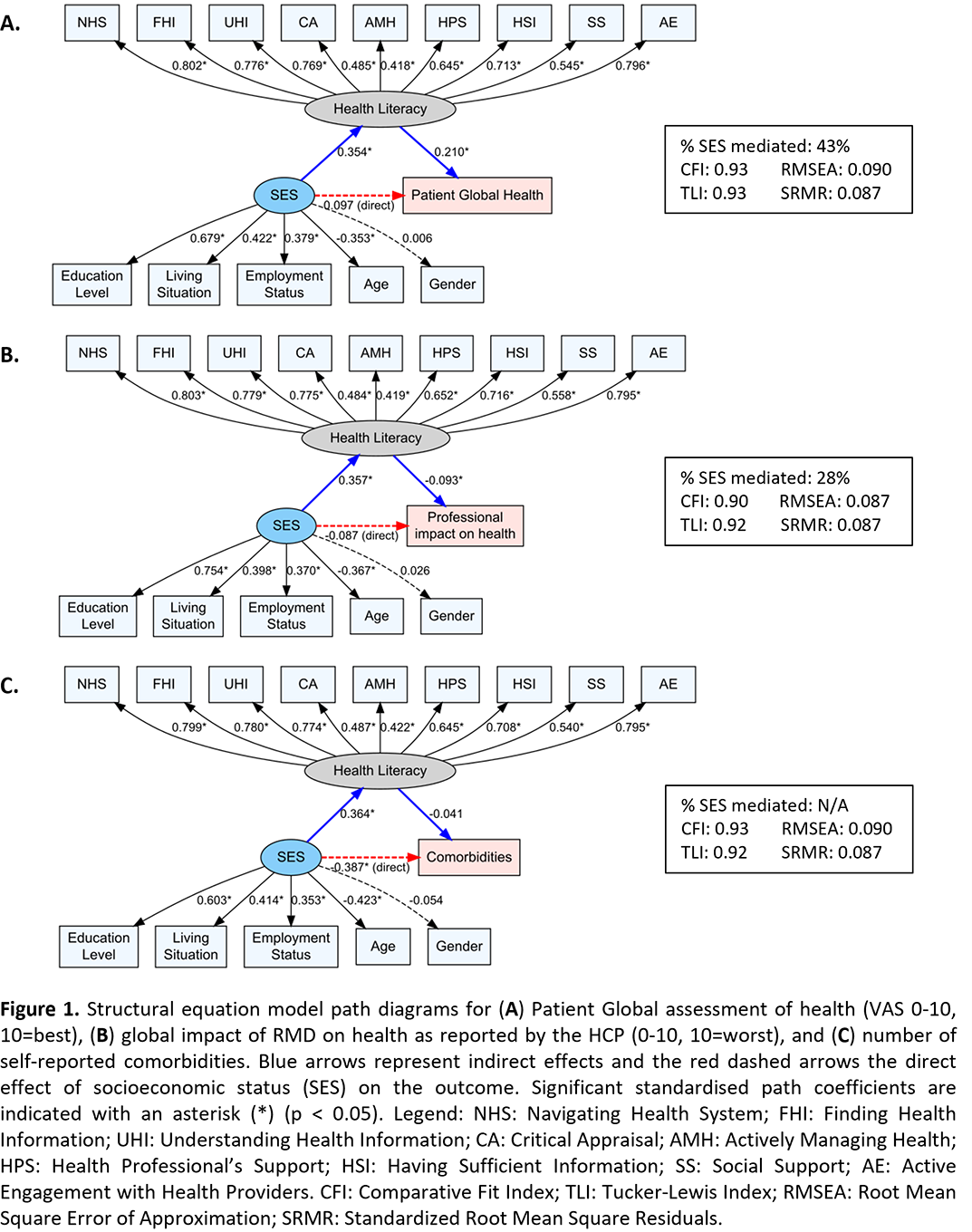
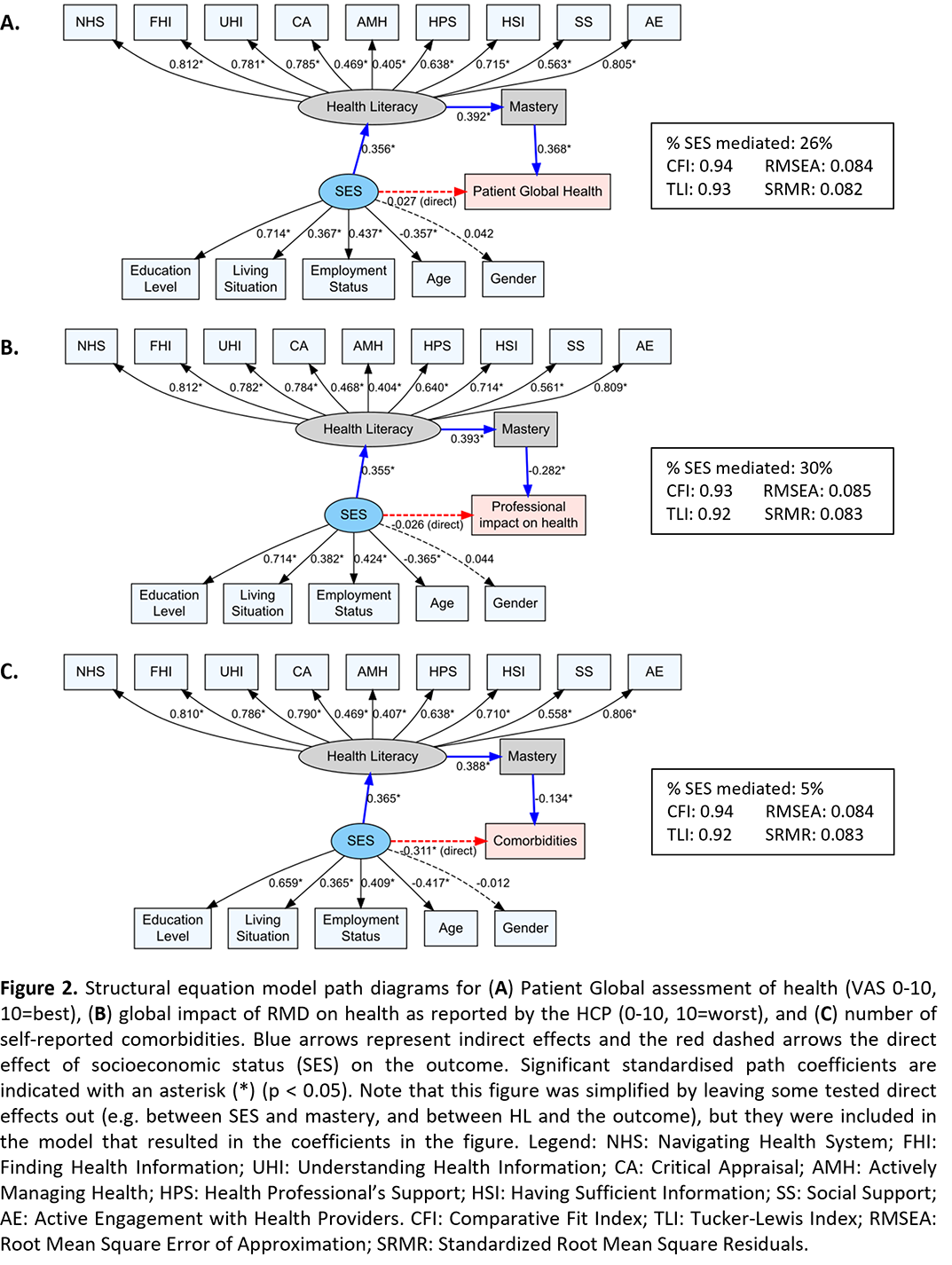
Results: 895 patients were included and HCP’s impact on health was available for 778 patients. Patients’ mean age was 61 years (SD 14), with 49% female, 51% low educational attainment, 82% native background, 75% living with children and/or partner and 35% employed (30% work disabled). Mean PtG health was 6.4 (SD:1.8), Mean HCP global on the impact of RMD on function 4.2 (3.5), and the number of comorbidities 1.2 (1.3; range 0-7). In the confirmatory factor analyses, migration status did not significantly contribute to the latent variable SES and was excluded. SES was significantly associated with each of the three outcomes. In the SEM, the overall indirect effect of SES through HL on either PtG health or HCP’s impact on health was significant, whereas the direct effect of SES on these outcomes became small and non-significant. Overall, 43% of the total effect of SES on PtG health (Figure 1A) and 28% of the total effect of SES on HCP’s impact on health (Figure 1B), was mediated through health literacy. For the number of comorbidities (Figure 1C), SES was also positively associated with HL. However, HL was not significantly associated with comorbidities, resulting in a non-significant indirect effect. This indicates that the relationship between SES and comorbidities operates primarily through a direct pathway rather than via health literacy. Fit parameters indicated a good model fit for each model. SEM with mastery as mediator showed similar patterns with a higher proportion mediated, when compared to HL (67% for PtG health) but substantially lower model fit. Models with sequential mediation confirmed mastery as an additional mediator but supressed the effect of HL (Figure 2). Education was the component most strongly contributing to SES, and Navigating the Healthcare System (HLQ domain 7) and Active Engagement with HCP (HLQ domain 6) were the components most strongly contributing to HL.
Conclusions: HL mediates the relationship between socioeconomic status (SES) and PtG health or HCP’s impact on health. Although mastery mediates an important part of the association between HL and these outcomes, the model fit worsened when adding mastery to the model with health literacy as the mediator, indicating relevant factors are missing. Interestingly, SES had a strong direct effect on comorbidities, but without evidence of mediation by HL or mastery. We hereby show, for the first time, that HL seems to be an actionable target to reduce the socio-economic health gap in rheumatology. Targeting healthy literacy may have impact on health outcomes, regardless the patient’s SES.
REFERENCES: [1] Bakker, M. Arthritis Care Res 2021.
[2] Gorter A. Rheumatology 2023.
[3] Paasche-Orlow M. & Wolf, M. Am J Health Behav 2007.
Acknowledgments: NIL.
Disclosure of Interests: Ayleen Mufudza: None declared, Mark Matthijs Bakker Eli Lilly, Sandoz, Eli Lilly, Sofia Ramiro Eli Lilly, AbbVie, Alfasigma, Johnson & Johnson, MSD, Novartis, Pfizer, Takeda, UCB, Eli Lilly, AbbVie, Alfasigma, MSD, Novartis, Pfizer, UCB, Annelies Agten: None declared, Annelies Boonen Johnson & Johnson, AbbVie, Pfizer, UCB, Eli Lilly, AbbVie.