fetching data ... 
Background: CD19-directed T cell engagers (TCE) achieve deep B cell depletion, and high-levels of efficacy across treatment-resistant autoimmune diseases. CLN-978 is a subcutaneously administered, CD19 x CD3 TCE. Studies of CLN-978 in cynomolgus monkeys showed profound B cell depletion below the level of detection in peripheral blood as well as lymphoid and other tissues. CLN-978 was previously administered to three patients with refractory B cell lymphoma, with complete response observed in one patient and an overall favorable safety profile.
Objectives: To evaluate the safety, pharmacokinetics, pharmacodynamics, and effects on disease activity of CLN-978 in two phase 1 studies of patients with treatment-refractory rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE).
Methods: OUTRACE RA enrolls RA patients with active (DAS28-ESR ≥ 3.2), refractory (failed ≥2 previous targeted treatments), and B cell-driven RA defined as either (i) seropositivity for RF and/or any anti-modified protein antibodies (AMPA) and/or (ii) synovial B cell infiltration. RA assessments include DAS28, synovial ultrasound (US), as well as synovial and lymph node biopsies if feasible (baseline and Week 4). OUTRACE SLE enrolls SLE patients with active (hSLEDAI ≥ 6), refractory (failed at least one biologic or immunosuppressive agent), and seropositive SLE. SLE assessments include the hSLEDAI, CLASI, and physician’s global assessment. CLN-978 is administered by subcutaneous injection, using a step-up dose on Day 1 (cohort 1) and a target dose on Day 8 (cohorts 2 and beyond). B cell counts and other immune cell subsets are assessed longitudinally in the peripheral blood.
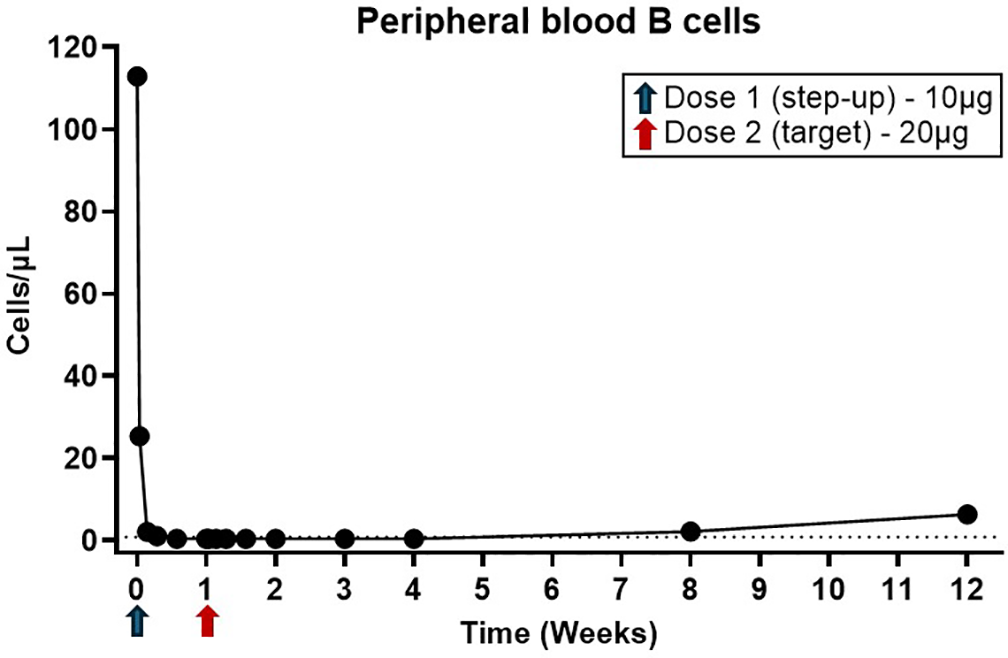
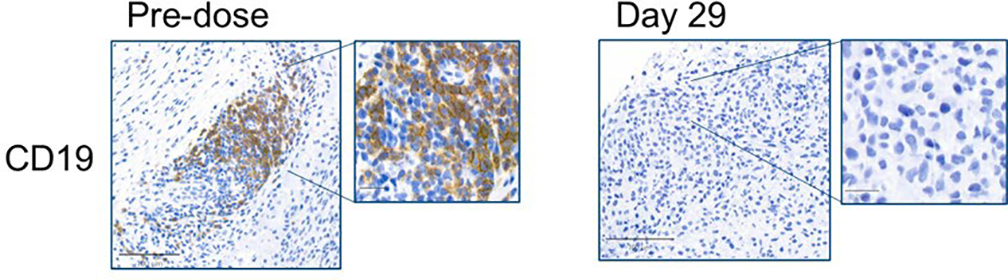
Results: As of 14 Jan 2026, 14 patients were dosed across the RA (cohorts 1-3, n=5) and SLE (cohorts 1-3, n=9) trials. All Day 1 (step up) doses were 10 mcg, and Day 8 target doses were 20 mcg (cohort 2) or 30 mcg (cohort 3). Cytokine release syndrome (CRS) occurred in 4 patients, was limited to Grade 1, and occurred within 24 hours of the 10 mcg step up dose. No CRS was reported after administration of any target dose. No cases of ICANS have been reported. Only one infection of Grade ≥2 occurred, a urinary tract infection, which resolved with antibiotic treatment. Injection site reactions occurred in 2 patients (Grade 1 and 2) following the 10 mcg step up dose. Following 10 mcg dosing, 9/11 patients exhibited depletion of B cells > 75% relative to baseline levels. Following 20 mcg dosing, 3/6 patients had depletion of B cells below the level of quantification, the other 3 patients exhibited decreases of 98.5%, 77%, and 64% relative to baseline levels. Depletion of CD19+ B cells below the level of detection in peripheral blood (Figure 1) and synovium (Figure 2) are shown for a patient treated in RA cohort 2 (20 mcg target dose). Transient decreases in peripheral blood T cell levels were observed, consistent with a known pharmacodynamic effect of T cell activation by TCEs. Among patients with at least 4 weeks of follow up data post-baseline, 4 of 5 RA patients had decrease in DAS28-ESR [including 4 of 4 patients decreasing from high activity (> 5.1) to moderate activity (3 patients) or remission (1 patient)], and 5 of 6 patients had decrease in SLEDAI score of ≥4 points. Ultrasound synovitis scores decreased in 3 of 4 RA patients.
Conclusions: CLN-978 was well tolerated and demonstrated a favorable safety profile in both RA and SLE patients. A single target dose of CLN-978 induced robust B cell depletion in both peripheral blood and tissues, with promising clinical efficacy in RA and SLE patients at the initial dose levels tested. Dose escalation continues in these studies, and updated data will be presented.
Reduction in absolute number of blood B cells (defined as the total number of CD19+CD20+, CD19+CD20-, and CD19-CD20+ cells) observed in an RA patient in Cohort 2. The dotted line represents the lower limit of quantitation.
Immunohistochemistry analysis of the synovial biopsy collected at baseline (pre-dose) and at week 4 (Day 29) stained with anti-CD19 antibody demonstrated a complete clearance of CD19+ B cells.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Ricardo Grieshaber-Bouyer Received speaker honoraria from AbbVie, Alfasigma, BMS, Cullinan, Gilead, Lilly, Novartis, Sanofi, UCB, Xencor. Grants: AstraZeneca, Boehringer Ingelheim Stiftung, Candid, Else Kröner-Fresenius-Stiftung, Kyverna, Lupus Research Alliance, Johnson & Johnson, Pfizer, Anca Dinu Askanase Investigator/Consultant with Abbvie, Amgen, AstraZeneca, Aurinia, Biogen, BMS, Idorsia, Janssen, Genentech, GSK, Mallinckrodt, NKARTA, Pfizer, Sanofi, UCB, Rob Will: None declared, Nedal Adi: None declared, Kwabena Ayesu: None declared, Adrian Reber Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, Yue Zhang Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, Sarai Faison Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, Todd Shearer Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, Irina Shapiro Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, stephen wax Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, Jeffrey Jones Holds stock/stock options in Cullinan Therapeutics, Inc, Employee of Cullinan Therapeutics, Inc, Maria Gabriella Raimondo: None declared, Carlo Tur: None declared, Stefano Alivernini: None declared, Georg Schett Received speaker’s honoraria from Novartis, Johnson & Johnson, BMS and UCB, Maria Antonietta D’ Agostino Received speaker’s honoraria from Abbvie, AstraZeneca, Amgen, BMS, Eli Lilly, Johnson & Johnson, Novartis, and UCB.