fetching data ... 
Background: Janus kinase inhibitors (JAKi) are effective treatments for immune-mediated inflammatory diseases (IMIDs). Concerns regarding the cardiovascular safety of JAKi emerged after the ORAL Surveillance trial, leading European regulatory authorities to recommend restricting JAKi use in patients at high cardiovascular risk or aged ≥ 65 years. However, data focusing on JAKi safety in elderly patients remain limited, highlighting the need for a dedicated study in this population with a higher baseline risk of adverse events.
Objectives: This study aimed to compare the risk of major adverse cardiovascular events (MACE) associated with JAKi versus TNFi therapies in patients with IMIDs aged ≥65 and ≥75 years.
Methods: Using the French health data system (SNDS), we included patients aged ≥ 65 years with rheumatoid arthritis (RA), inflammatory bowel diseases (IBD), or spondyloarthritis (SpA) initiating a targeted disease-modifying anti-rheumatic drug (tDMARD) from January 1, 2017 to June 30, 2023. The observation period ended on December 31, 2023. MACE were defined as myocardial infarction, stroke, or cardiovascular death. The effect of tDMARD therapeutic class, modeled as a time-dependent variable (TNFi, JAKi, other tDMARD or no tDMARD), on the risk of MACE was assessed using Cox proportional hazards models with dynamic inverse probability of treatment weighting. The propensity score included age, sex, comorbidities, traditional cardiovascular risk factors, surrogate markers of disease activity, prior treatment history and frailty. In addition to time-to-first-event analyses, recurrent MACE were analyzed using Lee Wei Amato models. The risk of MACE associated with JAKi versus TNFi therapies was also investigated in patients ≥ 75 years, according to IMID type, history of MACE, and calendar period (before vs after 2021, i.e., first ORAL Surveillance (ORAL-S) study results) and in patients similar to those included in ORAL Surveillance (ORAL-S population).
Results: A total of 29,252 elderly patients were included, 65.8% female, with a median age of 71 (IQR [68;76]) (Table 1). Most patients had RA (n=20 900, 71.4%) and 11,125 (38.0%) patients received a TNFi and 3,253 (11.1%) a JAKi at baseline. At 12 months, 3.2% and 12.1% of patients receiving a TNFi at the start of follow-up had switched to a JAKi and another tDMARD, respectively, and 19.2% had stopped their treatment. Patients receiving JAKi had a longer disease duration since initiation of the first tDMARD and a higher proportion had been treated with three or more prior tDMARD (19.9% vs.2.8%).
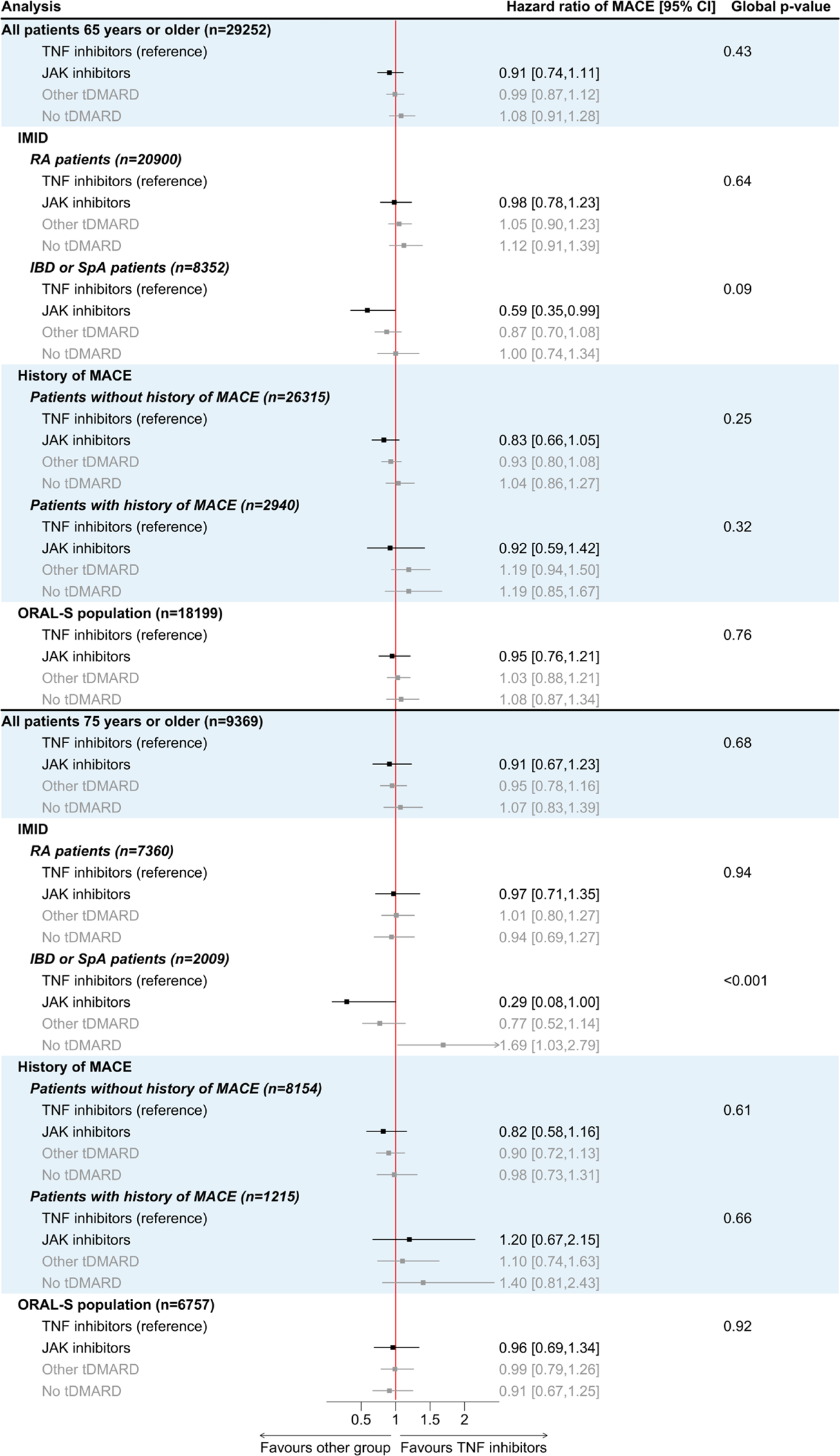
In time-to-first-event analyses, a total of 1,911 MACE occurred during follow-up: 703 strokes, 1,033 myocardial infarctions and 175 cardiovascular deaths. The 5-year crude cumulative incidence of MACE was 9.1% (95% confidence interval (CI), 8.2%–10.0%) among patients receiving TNFi and 9.2% (95% CI, 7.9%–10.5%) among those receiving JAKi. JAKi were not associated with an increased risk of MACE compared to TNFi in patients aged ≥65 years (weighted hazard ratio [wHR]: 0.91; 95% CI: 0.74-1.11) (Figure 1). Results were similar in recurrent events analysis (wHR: 0.89; 95% CI: 0.72-1.09), among RA patients (wHR: 0.98; 95% CI: 0.78-1.23), patients initiating their treatment before 2021 (wHR: 0.93; 95% CI: 0.72-1.19), and ORAL-S population (wHR: 0.95; 95% CI: 0.76-1.21). In contrast, a decreased risk of MACE was found among patients with IBD or SpA treated with JAKi (wHR: 0.59; 95% CI: 0.35-0.99). No statistically significant increase in risk was observed among patients with prior MACE (wHR: 0.92; 95% CI: 0.59–1.42). Results were similar in patients aged ≥75 years.
Conclusions: In this nationwide cohort of elderly patients with IMIDs, JAKi treatment did not increase the overall risk of major adverse cardiovascular events compared with TNFi, even among patients with prior MACE or specific risk factors. These findings suggest that age itself should not preclude the use of JAK inhibitors in clinical practice. Nevertheless, residual confounding cannot be excluded and individualized cardiovascular risk assessment remains essential, especially in patients with a history of cardiovascular events.
Baseline characteristics of the population initiating a TNF inhibitor or a JAK inhibitor at the start of the follow-up, before propensity score weighting (n=29 252)
| Characteristics | TNF inhibitor
| JAK inhibitor
| Total
|
|---|---|---|---|
| Age (years), median [IQR] | 71 [68;75] | 71 [67;75] | 71 [68;76] |
| Female sex | 7 232 (65.0) | 2 537 (78.0) | 19 251 (65.8) |
| Immune-mediated inflammatory disease | |||
| IBD | 1 179 (10.6) | 76 (2.3) | 3 716 (12.7) |
| Rheumatoid arthritis | 7 943 (71.4) | 2 991 (91.9) | 20 900 (71.4) |
| Spondyloarthritis | 2 003 (18.0) | 186 (5.7) | 4 636 (15.8) |
| Methotrexate in the last 6 months | 5 594 (50.3) | 1 508 (46.4) | 12 441 (42.5) |
| Number of prior tDMARD therapeutic class, median [IQR] | 0 [0;1] | 1 [0;2] | 1 [0;1] |
| Time (months) from the initiation of the first tDMARD, mean | 30.2 (48.5) | 67.7 (61.2) | 42.1 (54.9) |
| Obesity | 2 027 (18.2) | 648 (19.9) | 5 904 (20.2) |
| Smoking | 1 346 (12.1) | 398 (12.2) | 3 907 (13.4) |
| Diabetes | 1 968 (17.7) | 546 (16.8) | 5 698 (19.5) |
| Hypertension | 8 015 (72.0) | 2 388 (73.4) | 21 819 (74.6) |
| Dyslipidemia | 5 833 (52.4) | 1 731 (53.2) | 15 868 (54.2) |
| Peripheral artery disease | 1 584 (14.2) | 481 (14.8) | 4 858 (16.6) |
| Cerebrovascular disease | 740 (6.7) | 217 (6.7) | 2 245 (7.7) |
| Cancer | 1 764 (15.9) | 502 (15.4) | 6 255 (21.4) |
| Prior MACE | 948 (8.5) | 282 (8.7) | 2 937 (10.0) |
| Venous thromboembolism | 582 (5.2) | 180 (5.5) | 1 913 (6.5) |
Patients initiating a tDMARD other than JAKi or TNFi are not described, as this group comprises multiple therapeutic drug classes and lacks interpretability.
Comparison of MACE risk by tDMARD therapeutic class in patients aged ≥65 and ≥75 years, with dynamic inverse probability of treatment weighting
The number of included patients before weighting are shown for each analysis. Estimates for the “other tDMARD” and “no tDMARD” groups are shown in grey in the forest plot, as they are included in the models but are not of primary interest due to their limited interpretability.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Raphaelle Curmin: None declared, Bruno Fautrel AbbVie, Amgen, Biogen, BMS, Celltrion, Fresenius Kabi, Galapagos, Gilead, Janssen, Lilly, Medac, MSD, Nordic Pharma, Novartis, Pfizer, Roche, Sandoz, Sanofi- Genzyme, Sobi, UCB and Viatris, AbbVie, MSD and Pfizer, yann de-rycke: None declared, Thao Pham: None declared, Corinne Miceli Richard: None declared, Julien Kirchgesner Abbvie, Amgen, Alfasigma, Celltrion, Ferring, Galapagos, Janssen, Johnson & Johnson, Lilly, MSD, Takeda, Theradiag, Tillots, Pfizer, and Resilience, Florence Tubach F. Tubach is the head of the Pharmacoepidemiology Centre of the AP-HP and of the Clinical Research Unit of Pitie-Salpetriere Hospitals; both these structures have received research funding, grants and consultancy fees from Novartis, GSK and MSD. F. Tubach did not receive any personal remuneration from these companies.