fetching data ... 
Background: Despite guideline recommendations for routine bone mineral density (BMD) screening in older adults, uptake of dual-energy X-ray absorptiometry (DXA) remains low. Artificial intelligence (AI)-enabled analysis of routinely obtained computed tomography (CT) scans can provide opportunistic screening by estimating BMD from Hounsfield units (HU) at the spine or hip, potentially identifying high-risk patients who were not otherwise screened [1]. However, AI-enabled opportunistic screening has not been integrated into routine clinical workflows to expand BMD screening and inform treatment decisions among at-risk patients to facilitate population health screening. Further data are needed to inform feasibility and sample size estimates for interventions leveraging opportunistic CT to improve BMD screening uptake.
Objectives: To quantify DXA utilization and bone-active medication use among BMD-screening-eligible older adults without a prior osteoporosis diagnosis who were identified as at-risk using CT-based HU assessment.
Methods: This retrospective cohort study included women aged ≥65 and men aged ≥70 who underwent abdominal CT at a single institution from 2015-2018 and whose CT scans were suitable for lumbar vertebra (L1) HU assessment. We excluded CTs with hardware interfering with spinal imaging, and CTs from individuals with existing osteoporosis diagnosis or recent evaluation for osteoporosis defined as presence of: prior osteoporotic fracture ever, or receipt of DXA or bone-active medication use within the previous 3 years. We randomly selected 420 CTs (from a pool of 29,881 CTs) to undergo blinded processing for L1 HU assessment. Abdominal CT scans had been obtained for routine clinical indications across emergency, inpatient, outpatient, and procedural settings. For individuals with multiple eligible CTs, only the first randomly selected scan was included. As this was an observational study reflecting usual care, CT-based risk estimates were not disclosed and no actions were taken based on HU findings. Osteoporosis risk was classified as high-risk (L1 HU <135) or low-risk (L1 HU ≥135). This threshold was selected based on prior validation studies demonstrating ~75% sensitivity and specificity for osteoporosis and 90% sensitivity and 47% specificity for osteopenia [2,3]. We assessed outcomes over 8 years (through 2025) following the index CT including DXA (based on CPT codes) or bone-active medication use (i.e., use of bisphosphonates, denosumab, raloxifene, bazedoxifene, or anabolics). Covariates included demographics, clinical characteristics, and measures of social determinants of health. We used separate multivariable logistic regression models to compare the risk between the osteoporosis high-risk and low-risk groups for outcomes of DXA utilization or bone-active medication use following the CT, using the index CT as baseline and adjusting for covariates.
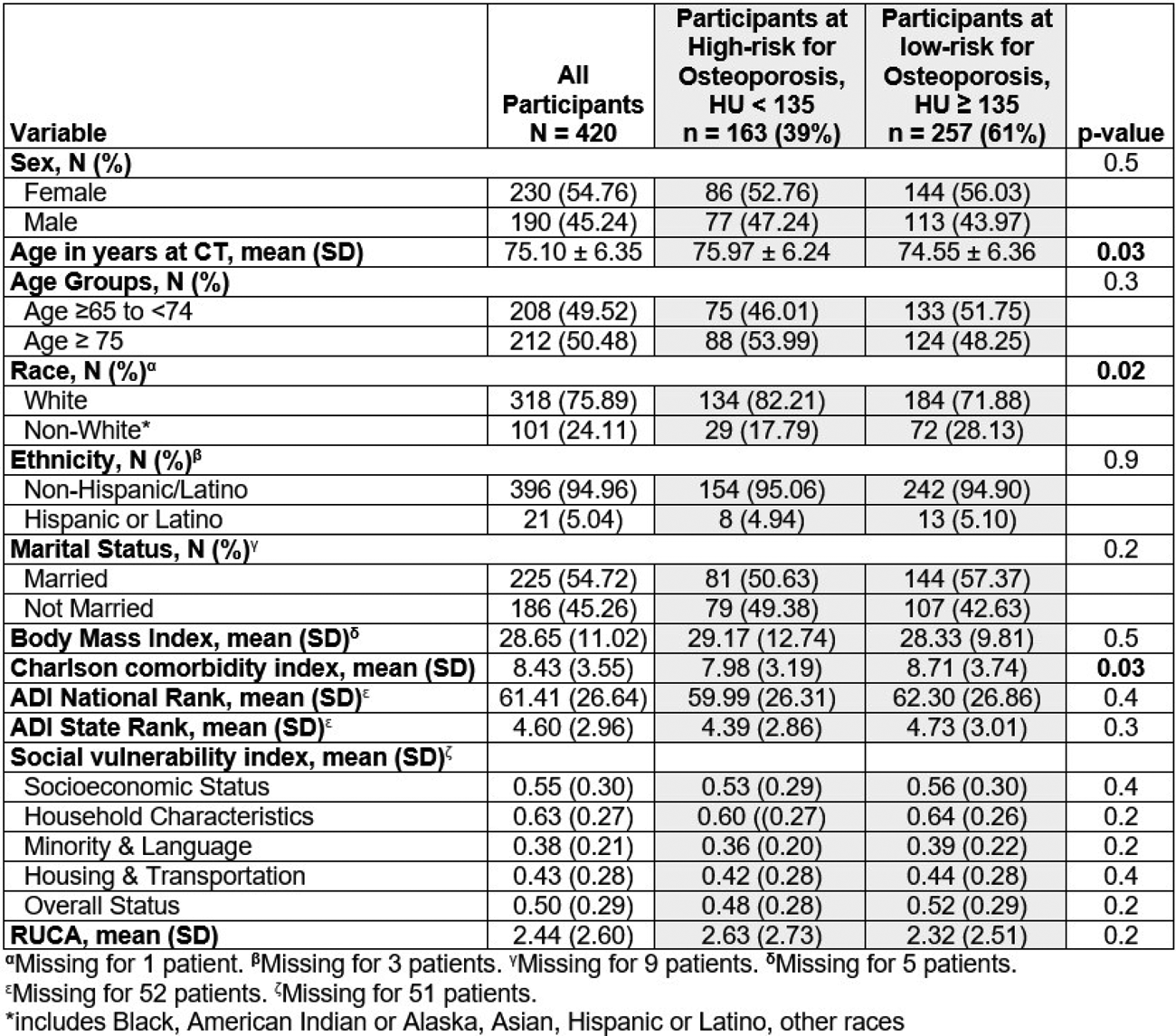
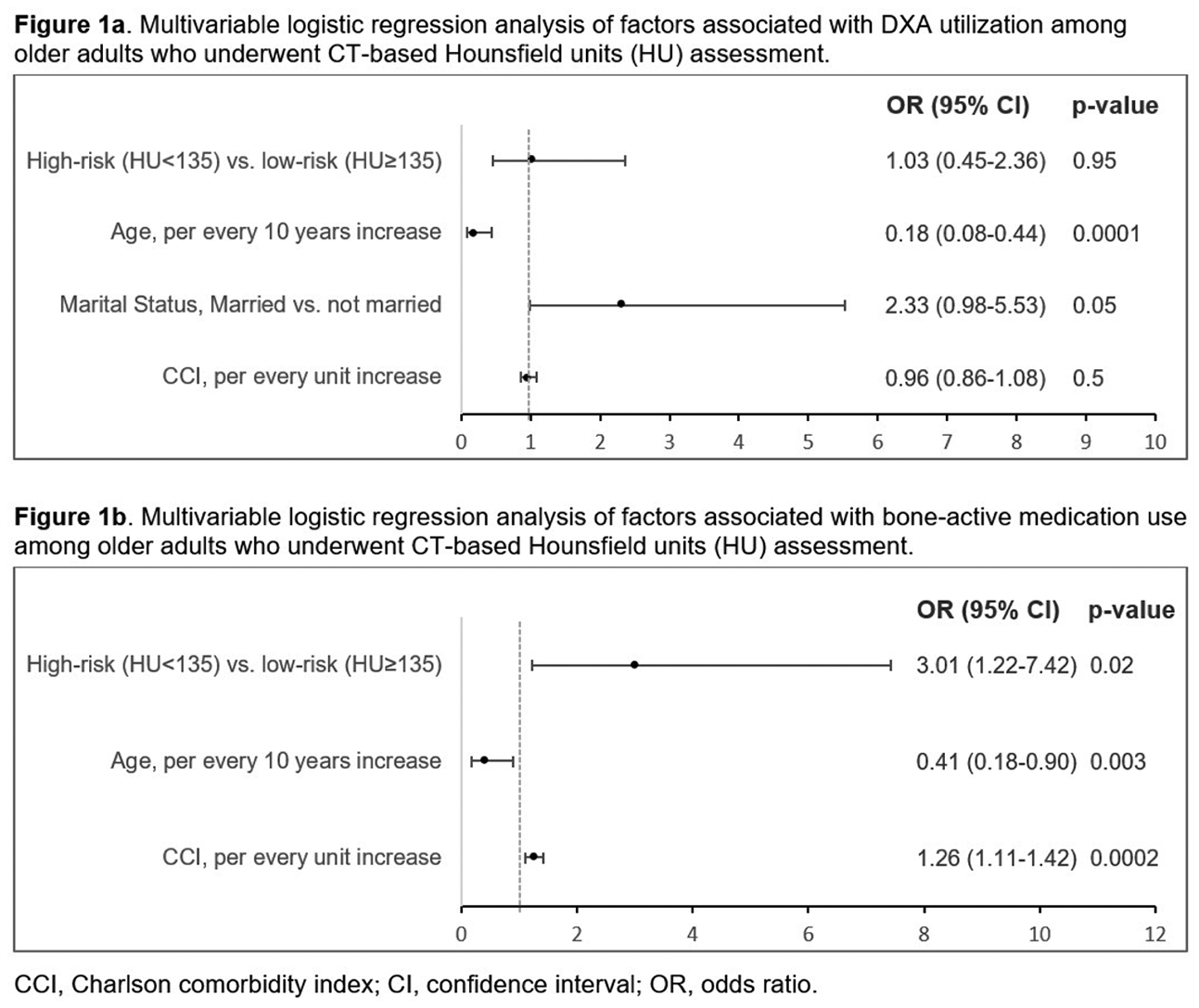
Results: Among 420 patients (mean [SD] age 75.1 ± 6.4 years; 55% female; 76% White race), 163 (39%) were classified as high-risk for osteoporosis ( Table 1 ). In the univariable analysis, there were significant differences in age, race, and CCI between risk groups ( Table 1 ). During follow-up, 30 patients (7%) underwent DXA and 24 (6%) used bone-active medications. Among patients classified as high-risk for osteoporosis, only 10 (6%) underwent DXA and 13 (8%) initiated bone-active medications during follow-up. Older age was associated with lower odds of receipt of DXA (OR=0.18, 95% CI 0.08-0.44, p=0.0001, for every 10-year increase) ( Figure 1a ). High-risk for osteoporosis (HU <135) was associated with higher odds of medication use compared with low-risk status (OR=3.01, 95% CI 1.22-7.42, p=0.02) ( Figure 1b ). In addition, older age was associated with lower odds of medication use (OR=0.41, 95% CI 0.18-0.90, p=0.003, for every 10-year increase), while greater comorbidity burden was associated with higher odds of medication use (CCI, OR=1.28, 95% CI 1.11-1.42, p=0.0002, for every 1-unit increase).
Conclusions: Among a sample of 420 BMD-screening eligible older adults without a prior diagnosis of osteoporosis and who underwent AI-enabled analysis for HU assessment, approximately 39% were characterized as high-risk for osteoporosis. Despite guidelines recommending routine BMD screening in women aged ≥65 and men aged ≥70, only 6% of high-risk patients underwent DXA during a 5-year follow-up period, highlighting substantial gaps in downstream evaluation. These data demonstrate preliminary feasibility of using AI-enabled CT-based opportunistic imaging to identify and characterize patients who may benefit from a future intervention focused on further osteoporosis screening efforts including DXA.
Table 1. Demographic characteristics of the study population including women aged ≥65 and men aged ≥70 who underwent abdominal CT from 2015-2018 with L1 Hounsfield units (HU) assessment.
REFERENCES: [1] Pickhardt PJ, et al. Improved CT-based Osteoporosis Assessment with a Fully Automated Deep Learning Tool. Radiol Artif Intell . Sep 2022;4(5):e220042. doi:10.1148/ryai.220042.
[2] Zaidi Q, et al. Measurement Techniques and Utility of Hounsfield Unit Values for Assessment of Bone Quality Prior to Spinal Instrumentation: A Review of Current Literature. Spine (Phila Pa 1976 ). Feb 15 2019;44(4):E239-E244.
[3] Pickhardt PJ, et al. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann Intern Med . Apr 16 2013;158(8):588-95.
Acknowledgments: NIL.
Disclosure of Interests: Lesley Jackson: None declared, Steven Rothenberg: None declared, Rahima Begum: None declared, Jeffrey R Curtis Amgen, Amgen, John Osborne: None declared, Navneet Baidwan: None declared, Vasil Bachiashvili: None declared, Kenneth Saag: None declared, Maria Danila Boehringer Ingelheim, Amgen.