fetching data ... 
Background: Long-term glucocorticoid (GC) use in older adults is associated with an increased risk of adverse events and GC avoidance or early discontinuation is recommended for rheumatoid arthritis (RA); however, real-world studies have shown that older patients are more likely to continue GC therapy than younger patients. Accordingly, treatment targets in late-onset RA (LORA) should incorporate not only disease activity control but also GC discontinuation.
Objectives: To identify predictors during the first 3 months of treatment for achieving GC-free remission at 12 months in methotrexate (MTX)-naïve patients with LORA diagnosed at ≥65 years of age, and to explore appropriate 3-month treatment targets.
Methods: This multicenter prospective cohort study enrolled patients with LORA who newly initiated conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) or biologic or targeted synthetic DMARDs (b/tsDMARDs) in the LORIS (Late-onset Rheumatoid Arthritis Registry Study) between January 2022 and March 2024. Of 246 registered patients, 22 were excluded due to withdrawal of consent, discontinuation of hospital visits, or loss to follow-up. The treatment target was remission or low disease activity (LDA). MTX was recommended as the first-line csDMARD in the protocol, and reasons for MTX non-use were prospectively recorded. Initiation of GC therapy was left to the discretion of the treating physician, with discontinuation recommended as early as possible; reasons for inability to discontinue GC were also documented. The primary endpoint was GC-free simplified disease activity index (SDAI) remission at 12 months. Secondary endpoints included GC-free LDA, remission, and LDA.
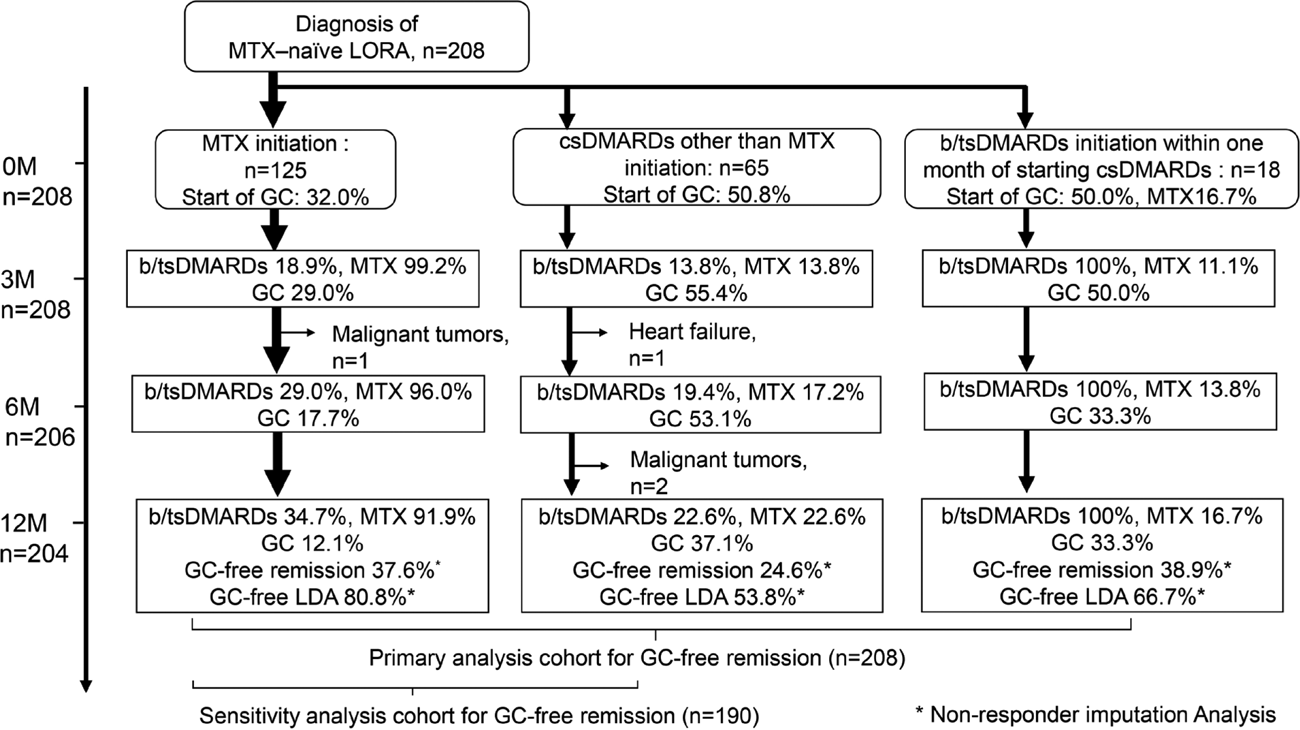
Results: At treatment initiation, 127 patients received MTX (MTX group), 63 received csDMARDs other than MTX (other csDMARDs group), and 18 initiated b/tsDMARDs within one month of starting csDMARDs (MTX use 16.7%; b/tsDMARDs group). Baseline GC use was 31.5%, 50.8%, and 50.0%, respectively. The proportions of MTX, b/tsDMARD, and GC use after 3 months are shown in Figure 1. The main reasons for MTX non-use were patient preference, renal dysfunction, history of malignancy, respiratory disease, and cognitive impairment. The most common reason for continued GC use at 3 or 6 months was insufficient disease activity control. At 12 months, GC-free remission was achieved in 37.6%, 24.6%, and 38.9%, while GC-free LDA in 80.8%, 53.8%, and 66.7% in the MTX, other csDMARDs, and b/tsDMARDs groups, respectively (Figure 1).
In the cohort for the primary analysis, patients who achieved GC-free remission at 12 months (n=70) and those who did not (n=138) showed comparable baseline age, sex, anti–citrullinated protein antibody positivity (42.9% vs 50.7%, p=0.283), Health Assessment Questionnaire Disability Index (1.182±0.832 vs 1.326±0.857, p=0.251), grip strength, smoking history, and prevalence of comorbidities including respiratory disease, cardiovascular disease, osteoporosis, and dementia. Baseline MTX use (67.1% vs 58.7%) and GC use (31.4% vs 43.5%) did not differ significantly between the groups.
At 3 months, both achievement of GC-free LDA and achievement of LDA overall were significantly more frequent among patients who achieved GC-free remission at 12 months than among those who did not (GC-free LDA: 55.7% vs 31.2%, p=0.001; LDA overall: 82.9% vs 55.8%, p= <0.001). Initiation of b/tsDMARDs within 3 months was also more frequent in the patients with GC-free remission at 12 months (34.3% vs 19.6%). b/tsDMARDs were subsequently used at 6 months (40.0% vs 27.5%) and 12 months (33.3% vs 41.4%).
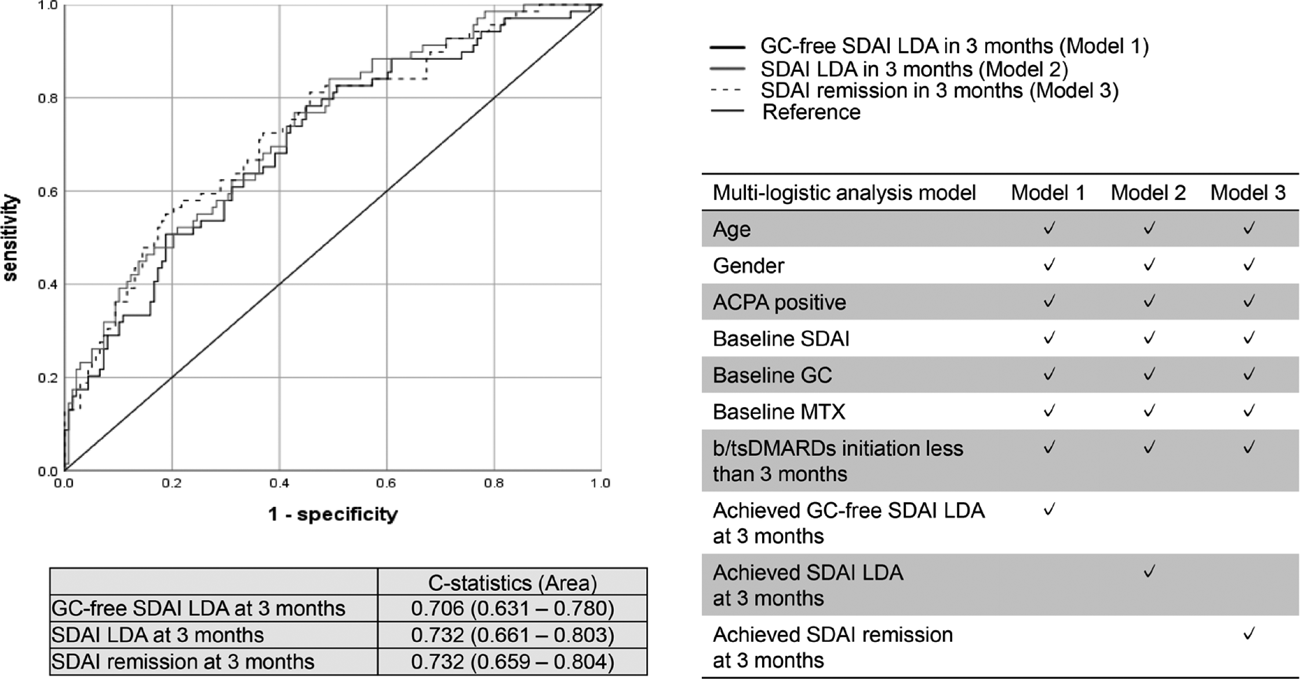
Three multivariable logistic regression models were evaluated (Figure 2). In Model 1, including age, sex, ACPA positivity, baseline SDAI, baseline GC use, baseline MTX use, initiation of b/tsDMARDs within 3 months, and achievement of GC-free SDAI LDA at 3 months, early initiation of b/tsDMARDs (adjusted odds ratio [aOR] 3.12, 95% confidence interval [CI] 1.46–6.67) and GC-free SDAI LDA at 3 months (aOR 2.93, 95% CI 1.40–6.15) were independent predictors of GC-free remission at 12 months. GC-free SDAI LDA at 3 months was replaced with SDAI LDA and SDAI remission at 3 months in Model 2 and 3, respectively. In these models, achievement of SDAI LDA at 3 months and SDAI remission at 3 months remained significant predictors (SDAI LDA, aOR 4.38, 95% CI 2.04–9.39; SDAI remission, aOR 4.86, 95% CI 2.27–10.4). Interestingly, the receiver operating characteristic (ROC) curves for Models 1, 2, and 3 largely overlapped. Comparison of predictive performance using C-statistics demonstrated good discrimination for predicting GC-free remission at 12 months across all three models, with area under the curve (AUC) values of 0.706 (95% CI 0.631–0.780) for Model 1, 0.732 (95% CI 0.661–0.803) for Model 2, and 0.732 (95% CI 0.659–0.804) for Model 3, indicating no difference in predictive ability among GC-free LDA (Model 1), LDA (Model 2), and SDAI remission at 3 months (Model 3) (Figure 2).
In a sensitivity analysis of 190 patients who initiated csDMARDs, Model 2 consistently showed that SDAI LDA at 3 months (aOR 3.65, 95%CI 1.66–8.03) and initiation of b/tsDMARDs within 3 months (aOR 3.58, 95%CI 1.51–8.48) were significant independent predictors. Similarly, the C-statistics of Models 1, 2, and 3 were comparable, and the ROC curves largely overlapped among the three groups.
Conclusions: In patients with LORA, achieving LDA at 3 months may be associated with subsequent attainment of GC–free remission at 12 months, even if GC-free status has not been achieved by 3 months. Early initiation of b/tsDMARDs within 3 months and setting LDA as the treatment target at 3 months appear to be useful strategies for achieving GC-free remission at 12 months.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Takahiko Sugihara TS has received speaker’s fee from Abbvie Japan Co., Ltd., AsahiKASEI Co., Ltd., Astellas Pharma Inc., Ayumi Pharmaceutical, Boehringer-Ingelheim Japan, Inc, Bristol Myers Squibb K.K., Chugai Pharmaceutical Co., Ltd., Eli Lilly Japan K.K., Kissei Pharmaceutical Co., Ltd., Mitsubishi-Tanabe Pharma Co., Ono Pharmaceutical, Pfizer Japan Inc., and Taisho Pharmaceutical Co., Ltd., TS has received research grants from AsahiKASEI Co., Ltd., Daiichi Sankyo., Chugai Pharmaceutical Co., Ltd., and Ono Pharmaceutical., Masayo Kojima Speakers bureau: AbbVie Inc., Astellas Pharma Inc., Ayumi Pharmaceutical Corporation, AstraZeneca plc, Chugai Pharmaceutical Co., Ltd., Sumitomo Pharma Co., Ltd., Eisai Co., Ltd., Eli Lilly and Company, Ono Pharmaceutical Co., Ltd., Pfizer Inc., Janssen Pharmaceutical Companies of Johnson & Johnson, Takeda Pharmaceutical Company Limited, Tanabe Pharma Corporation, and UCB S.A., Yutaka Kawahito Speakers bureau: Asahi Kasei Pharma Co., Ltd., AbbVie Japan GK, Astellas Pharma Inc., AstraZeneca plc., Ayumi Pharmaceutical Co., Boehringer Ingelheim Japan, Inc., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Eli Lilly Japan K.K., Ltd., Daiichi Sankyo., GlaxoSmithKline K.K., Janssen Pharmaceutical K.K., Kissei Pharmaceutical Co., Ltd., Mitsubishi-Tanabe Pharma Co., Nippon Kayaku Co., Ltd., Novartis Pharma K.K., Pfizer Japan Inc., Taisho Toyama Pharmaceutical Co., Ltd., UCB Japan Co. Ltd. and Viatris Pharmaceuticals Japan Inc., Grant/research support: Asahi KASEI Pharma Co.Ltd., and Chugai Pharmaceutical Co., Toshihisa Kojima Speakers bureau: AbbVie, Chugai Pharma, Bristol-Myers Squibb, Eli Lilly, Taisho, Eisai, Asahikasei, Grant/research support: AbbVie, Astellas Pharma, Chugai Pharma, Taisho, Kazuo Matsui Speakers bureau: AbbVie, Asahi-Kasei Pharma, Astellas, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Chugai, Eisai, Eli Lilly, Janssen, Kissei, Otsuka Pharmaceutical, Pfizer, Sanofi, Taisho, Tanabe Pharma, Hajime Ishikawa: None declared, Shintaro Hirata AbbVie, Speakers bureau: AbbVie, Asahi-Kasei Pharma, Astellas, AstraZeneca, Ayumi, Bristol Myers Squibb, Boehringer Ingelheim, Celltrion, Chugai, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead Sciences, Glaxo SmithKline, Janssen, Nihon-Shinyaku, Novartis, Otsuka Pharmaceutical, Pfizer, Sandoz, Taisho, Tanabe Pharma, UCB, Consultant: Eisai, UCB, Grant/research support: Asahi-Kasei Pharma, Chugai, Otsuka, Taisho, Yuko Kaneko Speakers bureau: AbbVie, Asahi Kasei, Astellas, Boehringer Ingelheim, Bristol-Myers Squib, Chugai, Daiichi Sankyo, Eisai, Eli Lilly Japan K.K., Gilead, Janssen, Mitsubishi Pharma, Novartis, Pfizer, Taisho, UCB, Consultant: AbbVie, Asahi Kasei, Astellas, Boehringer Ingelheim, Bristol-Myers Squib, Chugai, Eli Lilly Japan K.K., Grant/research support: AbbVie, Asahi Kasei, Ayumi, Boehringer Ingelheim, Chugai, Eisai, Eli Lilly Japan K.K., Gilead, Mitsubishi Tanabe, Pfizer, Eiichi Tanaka Speakers bureau: AbbVie Japan GK, Asahi Kasei Corp., Astellas Pharma Inc., Ayumi Pharmaceutical Co., Boehringer Ingelheim Japan, Inc., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., Gilead Sciences, Inc., GlaxoSmithKline K.K., Mikasa Seiyaku co., Ltd., Mitsubishi Tanabe Pharma Co., Nichi-Iko Pharmaceutical Co., Ltd., Nippon Kayaku Co., Ltd., Pfizer Japan Inc, Sandoz K.K., Taisho Pharmaceutical Co., Ltd, Takeda Pharmaceutical Co., Ltd, Towa Pharmaceutical Co., Ltd., UCB Japan Co. Ltd. and Viatris Inc., Grant/research support: Pfizer Inc., Mitsumasa Kishimoto Received consulting fees and/or honoraria from AbbVie, Amgen, AstraZeneca, Asahi-Kasei Pharma,Ayumi Pharma, BMS, Chugai, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, Janssen, Novartis, Takeda, Tanabe-Mitsubishi, and UCB Pharma., Akio Morinobu Speakers bureau: Astellas, Bristol Myers Squibb, Chugai, Eisai, Eli Lilly, Grant/research support: Asahi-Kasei Pharma, Chugai, Taisho,Eizai, Tanabe pharma, Motomu Hashimoto Speakers bureau: Asahi Kasei, Astellas, AstraZeneca, Ayumi Pharma, Brystol Meyers, Chugai, Eisai, Eli Lilly, Gilead Sciences Japan, Janssen pharma, Ono Pharma, Tanabe Mitsubishi, UCB Japan, Grant/research support: Asahi Kasei, Astellas, Brystol Meyers, Eisai, Gilead Sciences Japan, Ohtsuka Pharma, Taisho Pharma, Towa Pharma, Isao Matsushita Speakers bureau: Eisai Co.,Ltd and AbbVie Inc., Toshihiko Hidaka Speakers bureau: AbbVie, Eli Lilly, Pfizer, Asahi-Kasei, Bristol-Myers Squibb, Chugai, Janssen, Taisho, Eisai., Keiichiro Nishida Speakers bureau: Asahi Kasei Pharma Corporation, AYUMI Pharmaceutical Corporation, Eisai Co., Ltd., ONO PHARMACEUTICAL CO., LTD., Daiichi Sankyo Company, Limited, Chugai Pharmaceutical Co., Ltd., Eli Lilly Japan K.K., Pfizer Japan Inc., Janssen Pharmaceutical K.K, Grant/research support: AbbVie GK, Chugai Pharmaceutical Co., Ltd., Hiromu Ito: None declared, Toshihiro Matsui Speakers bureau: Abbvie, AsahiKASEI, Astellas Pharma, Ayumi, Chugai, Daiichi Sankyo., Eli Lilly, Mitsubishi-Tanabe., Ono, Pfizer., Takeda, Taisho, and UCB., Grant/research support: AsahiKASEI, Chugai, Ryozo Harada Speakers bureau: AbbVie Japan GK, Asahi Kasei Corp., Astellas Pharma Inc., Ayumi Pharmaceutical Co., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., Taisho Pharmaceutical Co., Ltd, UCB Japan Co. Ltd. and Avanos Medical, Inc., Asami Abe Speakers bureau: AbbVie, Michinori Ishitoku Paid instructor: Asahi-Kasei Pharma, Chugai, Speakers bureau: AbbVie, Asahi-Kasei Pharma, Chugai, Otsuka Pharmaceutical, Tanabe-Mitsubishi, and Astellas, Takashi Kida Paid instructor: Asahi Kasei Pharma, Speakers bureau: Eisai and Mitsubishi Tanabe Pharma., Satoshi Takanashi: None declared, Keizo Maeda: None declared, Akira Onishi Speakers bureau: Pfizer Inc., Bristol Myers Squibb, Asahi Kasei Pharma Corp., Chugai Pharmaceutical Co. Ltd., Eli Lilly Japan K. K., UCB Japan Co., Mitsubishi Tanabe Pharma Co., Eisai Co. Ltd., AbbVie Inc., Taisho Pharmaceutical Co. Ltd., and Daiichi Sankyo Co, Ltd. Ltd., Grant/research support: Pfizer Inc., Bristol Myers Squibb, and Taisho Pharmaceutical Co. Ltd, Shuji Asai AbbVie, Eisai, and Eli Lilly., Astellas and UCB Japan., Toshihiro Nanki Ono Pharmaceutical Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Astellas Pharma Inc., Janssen Pharmaceutical K.K., Pfizer Japan Inc., Asahi Kasei Pharma Corp., Eli Lilly Japan K.K., AbbVie GK, Ayumi Pharmaceutical Corp., Daiichi Sankyo Co., Ltd., Mitsubishi Tanabe Pharma Corp., UCB Japan Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., AstraZeneca K.K., GlaxoSmithKline plc., Novartis Pharma K.K., Otsuka Pharmaceutical Co., Ltd., Nippon Kayaku Co., Ltd., Kissei Pharmaceutical Co., Ltd., Taisho Pharmaceutical Co., Ltd., UCB Japan Co., Ltd., Eisai Co., Ltd., Chugai Pharmaceutical Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., Asahi Kasei Pharma Corp., Mitsubishi Tanabe Pharma Corp., Ayumi Pharmaceutical Corp., Nippon Kayaku Co., Ltd., AbbVie GK, Taisho Pharmaceutical Co., Ltd., Nippon Boehringer Ingelheim Co., Ltd., Shionogi & Co., Ltd., Masayoshi Harigai Speakers bureau: AbbVie Japan GK, Asahi Kasei Corp., Ayumi Pharmaceutical Co., Boehringer Ingelheim Japan, Inc., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan K.K., Gilead Sciences Inc., Mitsubishi Tanabe Pharma Co., Mochida Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Pfizer Japan Inc., and Taisho Pharmaceutical Co., Ltd., Consultant: AbbVie, Boehringer-ingelheim, Bristol Myers Squibb Co., and Eli Lilly Japan K K., Grant/research support: AbbVie Japan GK, Asahi Kasei Corp., Ayumi Pharmaceutical Co., Boehringer Ingelheim Japan, Inc., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Eisai Co., Ltd., Eli Lilly Japan K.K., Mitsubishi Tanabe Pharma Co., Mochida Pharmaceutical Co., Ltd., Nippon Kayaku Co., Ltd., Pfizer Japan Inc., Taisho Pharmaceutical Co., Ltd., Teijin Pharma Ltd., UCB Japan Co., Ltd., and Viatris Japan.