fetching data ... 
Background: Response to targeted therapies in rheumatoid arthritis (RA) is heterogeneous and incompletely predicted by clinical features. Synovial biopsy studies have demonstrated that distinct patterns of synovial histomorphology, hypothesized to represent “pathotypes” (including lymphoid-rich, myeloid-dominant, and pauci-immune/fibroid states) show associations with differential therapeutic responses, however access to synovial tissue is not routinely practicable.
Objectives: To determine whether circulating active chromatin biomarkers identify gene activity, including genes previously reported from synovial biopsy studies, associated with clinical response to treatment across multiple drug classes, with a view to investigating the potential of these blood-based biomarkers to inform treatment choice in the management of RA.
Methods: An interim analysis was performed using baseline plasma samples from adults with established RA enrolled in PRIMA-102 (NCT05936970), a prospective, multicenter observational cohort of participants with moderate to high disease activity who initiated treatment with biologic or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) after inadequate response to prior therapy. Participants were classified as responders based on achievement of a minimal clinically important difference (MCID) in the Clinical Disease Activity Index (CDAI) at 12 weeks post-treatment. Plasma was processed using a novel assay that enriches for cell-free DNA fragments derived from active chromatin (cfDNA ac ). Enriched fragments were sequenced and mapped to the genome to generate normalized promoter-level counts across approximately 37,000 promoters, reflecting relative regulatory activity associated with gene transcription. Differential regulation between responders and non-responders was assessed within each drug class using multivariable linear modeling of normalized promoter-level cfDNA ac counts with control for multiple testing using false discovery rate (FDR). Unsupervised hierarchical clustering and pathway-level aggregation of differentially regulated promoters were used to assess responder–non-responder separation and concordance with published synovial transcriptomic pathotype signatures.
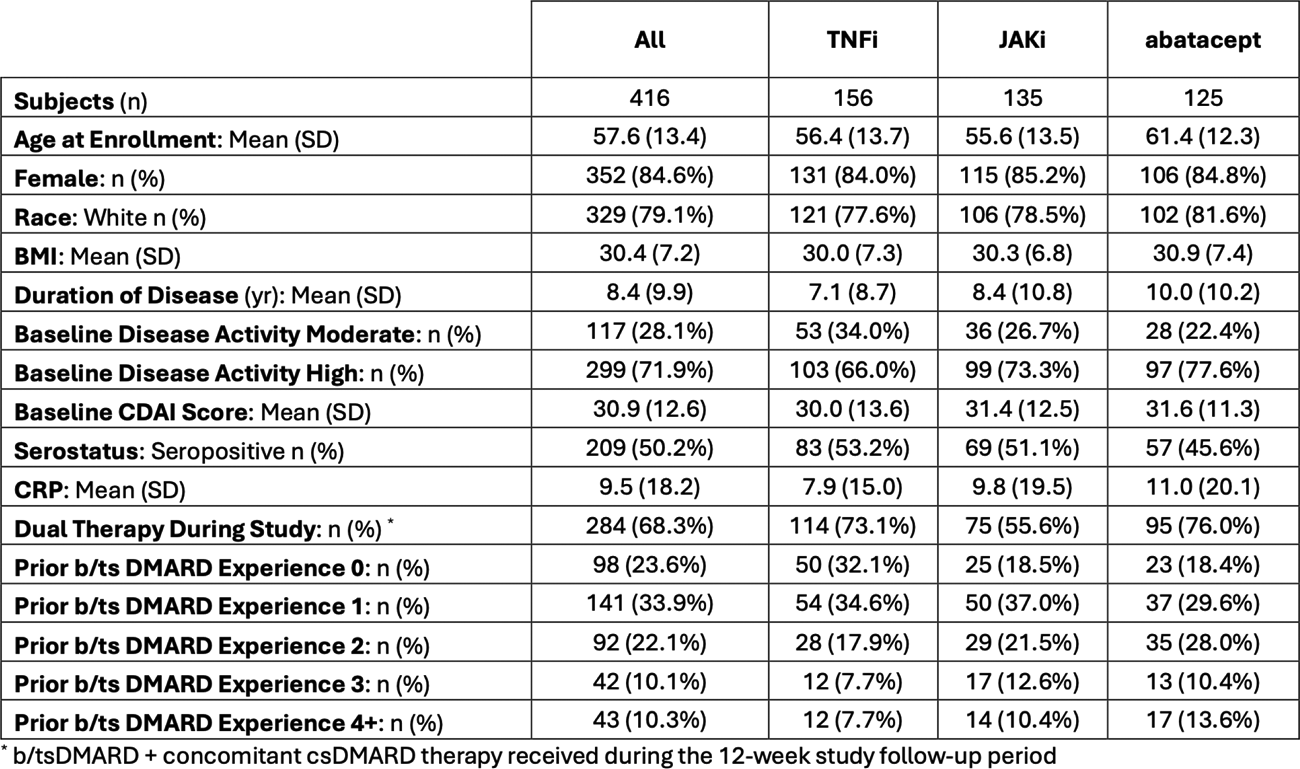
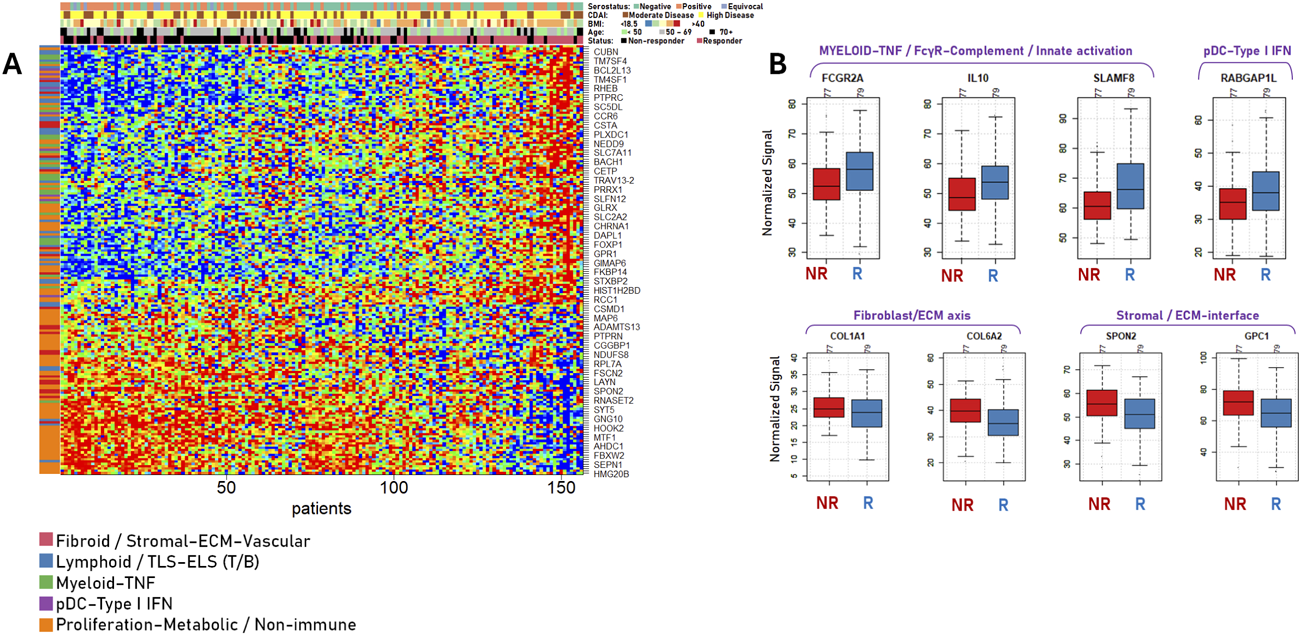
Results: Of the 416 participants in the analysis, 156 initiated on-study TNF inhibitors (TNFi), 135 initiated JAK inhibitors (JAKi), and 125 initiated abatacept (n = 125). 23.6% of the participants were b/tsDMARD-naïve. The mean age was 57.6 years, and the mean disease duration was 8.4 years (Table 1). 221 (53%) participants selected for analysis achieved response at 12 weeks. Response-associated promoter signals comprised 189 upregulated and 122 downregulated features for TNFi, 71 upregulated and 74 downregulated features for JAKi, and 61 upregulated and 127 downregulated features for abatacept. Cross-drug-class comparisons demonstrated limited overlap between response-associated promoter signatures (Jaccard indices <0.10 for all pairwise comparisons), with consistent directionality among overlapping genes, indicating largely class-specific baseline regulatory programs. TNFi responders showed significantly increased promoter signal for immune-associated genes including FCGR2A, C3AR1, MS4A1, and CCR6 (FDR <0.05), while non-responders demonstrated higher signal at stromal and extracellular matrix–associated loci (COL1A1, COL6A2, VCAN, CX3CL1), consistent with fibroid synovial biomarkers (Figure 1). These biomarkers overlapped directionally with previously described immune-rich versus pauci-immune synovial pathotypes. In JAKi-treated participants, responder-associated signals were enriched at promoters involved in cytokine signaling integration and transcriptional regulation, including PIK3R1, RASGRP3, LUC7L2, and mitochondrial regulatory loci (NDUFB6, MRPL2). Non-responders showed increased promoter signals at antigen-presenting cell and inhibitory myeloid loci (LAMP3, LILRB4, SIRPA, ACP5). These biomarkers partially overlapped with inflammatory synovial macrophage and dendritic cell signatures reported in published synovial biopsy studies. Abatacept responders demonstrated relative enrichment of adaptive immune regulatory loci (RTKN2, RGS2, DEAF1), consistent with less chronically activated immune states, whereas non-response was associated with increased regulatory signals at myeloid and fibroblast–macrophage interaction loci (C1QA, GPNMB, IL23A, ADAMTS5). cfDNA ac signatures showed consistent directionality with established synovial pathotypes across all three drug classes (χ 2 p < 10 -18 for each class), with large effect sizes (Cramér’s V ≈ 0.85–0.88), indicating strong alignment between response-associated cfDNA ac profiles and known lymphoid, myeloid, fibroid, and low-inflammatory synovial biomarkers.
Conclusions: Baseline plasma cfDNA ac profiling captures biologically meaningful biomarkers associated with response and non-response to TNFi, JAKi, and abatacept that are concordant with previously reported synovial tissue biomarker profiles, and largely distinct by drug class. These findings support the potential utility of circulating active chromatin signals for reflecting tissue-relevant biology and informing potential RA disease subtypes which could be used for patient stratification in clinical trials and treatment selection in RA.
Table 1. Demographics and patient characteristics
Baseline cfDNA promoter signatures associated with TNFi response
(A) Heatmap of baseline cfDNA promoter signals differing between responders and non-responders (FDR < 0.05). Rows denote promoters and columns denote patients. (B) Boxplots of selected cfDNA promoter biomarkers stratified by TNFi response status.
REFERENCES: [1] Triaille C, et al. Lancet Rheumatol. 2026;8:e66–e73.
[2] Dennis G Jr, et al. Ann Rheum Dis. 2014;73:129–137.
[3] Humby F, et al. Ann Rheum Dis. 2019;78:761–772.
[4] Pitzalis C, et al. Nat Rev Rheumatol. 2020;16:590-599.
[5] Lewis MJ, et al. Cell Rep. 2019;28:2455–2470.
[6] Smyth GK. Stat Appl Genet Mol Biol. 2004;3:Article 3.
Acknowledgments: NIL.
Disclosure of Interests: Kevin Lai: None declared, Jason Carlson: None declared, Shirley Vu: None declared, Kathy Lam: None declared, Diana Abdueva: None declared, Jeffrey R Curtis AbbVie, Amgen, Aqtual, BMS, CorEvitas, GSK, Janssen, Lilly, Moderna, Novartis, Pfizer, Sanofi, Scipher, Setpoint, TNacity Blue Ocean, UCB, AbbVie, Amgen, Aqtual, BMS, CorEvitas, GSK, Janssen, Lilly, Moderna, Novartis, Pfizer, Sanofi, Scipher, Setpoint, UCB, Peter C. Taylor AbbVie, Aqtual Inc., Alfasigma, Gilead, Takeda, Lilly, Nordic Pharma, Sanofi, UCB, Immunovant, ZuraBIo Inc., Moonlake, Alfasigma.