fetching data ... 
Background: Our recent work identified joint involvement patterns (JIP) as key discriminators, defining four subgroups along joint count and anatomical region (JIP-feet, JIP-oligo, JIP-hand, JIP-poly) [1]. These JIPs differed in treatment response and synovial histology, yet—as with other proposed RA subsets [2]—it remains unclear whether they represent distinct entities or disease stages [3]. To address this gap, we designed a post-hoc study to evaluate the stability and evolution of these baseline joint patterns and developed a method to assess within-subset coherency despite treatment-driven changes.
Objectives: (1) Determine the temporal stability of JIPs by assessing whether patients with the same baseline JIP remain similar during follow-up (2) assess how the number of affected joints change.
Methods: We analyzed three independent DMARD-naive early RA cohorts: 508 BeSt trial patients (446 with complete follow-up data) [4], 472 NORD-STAR trial patients (Swedish and Finnish cohorts only) [5, 6], and 515 Reumazorg Zuidwest Nederland (RZWN) registry patients (303 with complete data). Longitudinal data were collected at baseline and months 3, 6, 9, and 12 for the BeSt and RZWN cohorts, while NORD-STAR included all time points except the 9-month assessment. We used the parametric Leiden patient embedding of our original study, in which we previously discovered the four recurrent joint patterns [1], as a reference to assign patients from BeSt, NORD-STAR and RZWN to one of the four JIP subsets. To determine whether patients with similar baseline JIP consistently group together regardless of treatment initiation, we tracked how often they remained clustered with the same patients across multiple visits within 1 year. Specifically, we used the silhouette score to assess whether patients consistently clustered with their “original neighbors”—the 50 patients (k=50) who had the most similar joint involvement patterns at baseline. The silhouette score ranges from -1 to 1, with the latter representing perfect coherence (i.e. patient is similar to its own joint pattern) and the former total incoherence (more similar to different joint pattern). In real-world data, silhouette scores of 1 are extremely unlikely: scores ≥0.5 indicate great separability and ≥0.25 reasonable separability [9,10]. Finally, we tracked tender and swollen joint counts to assess the overall impact of treatment on joint involvement.
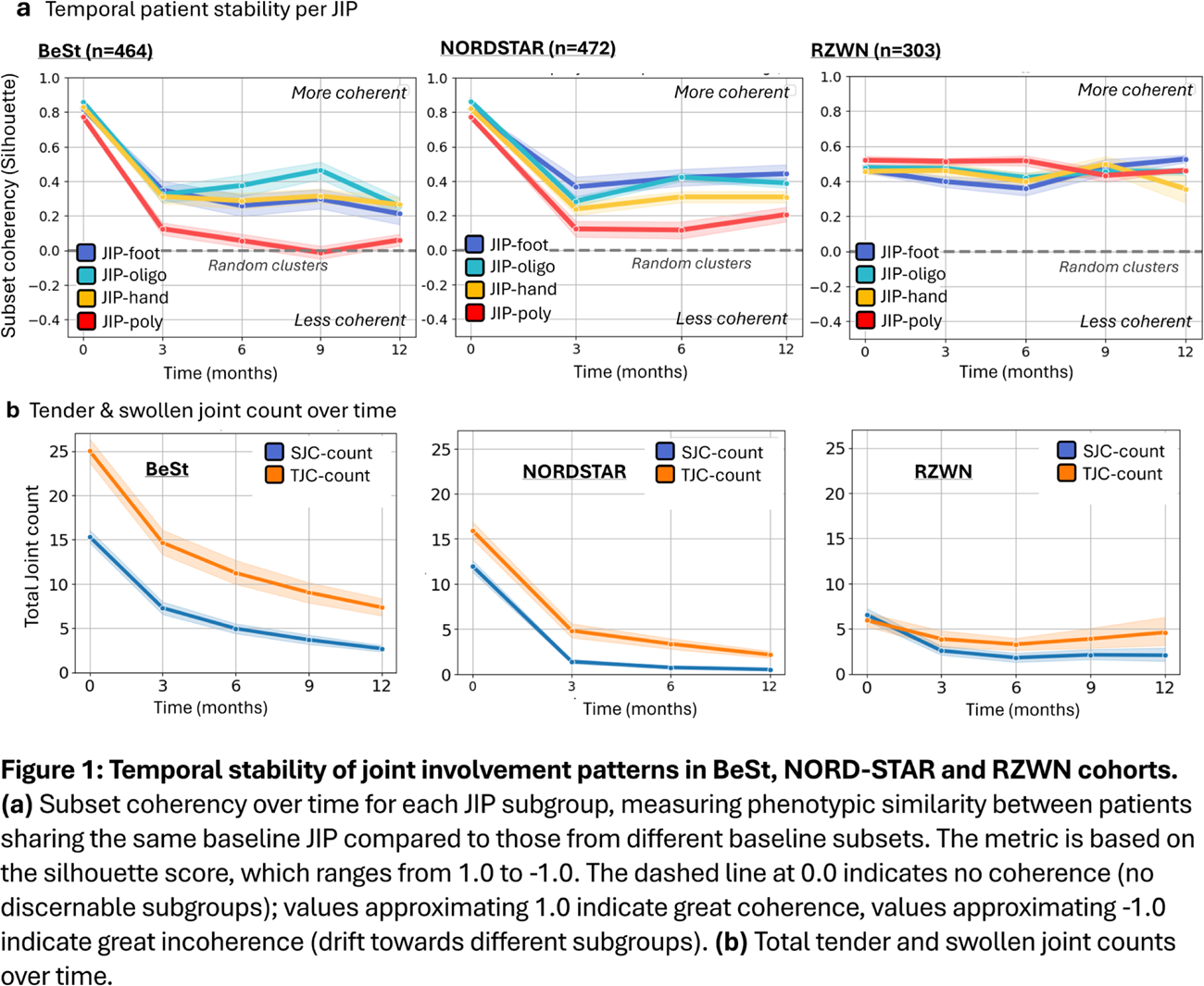
Results: As expected, the subset coherence was highest at baseline in all three cohorts (Figure 1A). In the trial data we found the highest silhouette scores around 0.80 for both NORDSTAR & BeSt. The real-world hospital cohort of RZWN had slightly lower silhouette scores around 0.50, possibly reflecting the lower joint counts causing more overlap between JIPs (Figure 1B). After treatment initiation, joint counts decreased across all cohorts, though mainly for swelling in RZWN. These treatment-related changes were also reflected by an initial drop in silhouette scores across the trial populations, as clinical differences between JIP subgroups became smaller. Nevertheless, we observe a persistent subset coherency. Mean silhouette scores at one year (SS≈0.25 for BeST and SS≈0.30 for NORDSTAR) demonstrated that patients continued to cluster more closely with their “baseline neighbors”—those who shared similar joint involvement patterns at baseline—than with patients from other JIP subgroups. The sole exception was the JIP-poly subgroup, in which patients progressively diverged from their baseline neighbors during follow-up. In the real world data of RZWN, the temporal coherence stayed more or less the same. In contrast to the trial populations, cluster coherency did not seem to decline after introduction of treatment, as patients persistently clustered with others who had comparable baseline JIP profiles (mean silhouette score of 0.50), suggesting these joint patterns are better preserved.
Conclusions: Even though therapeutic interventions effectively reduce overall joint counts, patients with similar joint involvement patterns at baseline continue to resemble each other more closely than patients with different baseline JIPs. This temporal stability indicates that baseline JIPs represent distinct and persistent subtypes, rather than representing transient disease states that all patients could move through. The JIP-poly subgroup being the only exception based on the trial data. Furthermore, the persistence of these joint patterns appeared to differ between the real-world and trial populations, likely reflecting differences in treatment intensity and selection criteria. Future work will focus on how different treatment strategies and patient populations impact temporal stability, and whether certain anatomical regions or joints show more recurrence over time than others, building on Heckert’s et al previous findings on local joint recurrence [7]. We have made our temporal dynamics method publicly available on GitHub to support researchers in assessing the stability of clinical signatures and patient subsets in treat-to-target settings [8].
REFERENCES: [1] Maarseveen et al. NPJ Digit Med. 2025 Oct 23;8(1):623.
[2] Lewis et al. Cell Rep . 2019;28(9):2455-2470.e5.
[3] Triaille et al. Lancet Rheumatol . 2026;8(1):e66-e73.
[4] Goekoop-Ruiterman et al. Arthritis Rheum . 2005;52(11):3381-3390.
[5] Hetland et al. BMJ 2020;371:m4328.
[6] Østergaard et al. Ann Rheum Dis. 2023;82:1286–1295.
[7] Heckert et al. Ann Rheum Dis . 2022;81(2):169-174.
[8] Github : github.com/levrex/Temporal_analysis_subsets.
[9] Dalmaijer et al. BMC Bioinformatics. 2022 May 31;23:205.
[10] Struyf et al. Comp Stat & Data An , 1997 Feb 26(1):17-37.
Acknowledgments: NIL.
Disclosure of Interests: None declared.