fetching data ... 
Background: Rheumatoid arthritis (RA) flares remain common despite advances in treat-to-target strategies, affecting 30–40% of patients annually, even in remission or low disease activity. Flares drive structural progression, functional decline, increased healthcare use and diminished quality of life. Although several prediction models have been developed in Europe and North America, no externally validated tools exist for Latin American populations, which present distinct epidemiological, socioeconomic and treatment-access profiles. Reliable flare prediction could enable preventive therapeutic adjustments, closer monitoring and more efficient allocation of limited healthcare resources.
Objectives: To develop, externally validate and digitally implement RheumaPredict , an ensemble machine learning model for individualized prediction of RA flares at 3–6 months using only routinely collected clinical, laboratory and treatment variables relevant to Latin American healthcare settings.
Methods: Following TRIPOD guidelines, clinical longitudinal data from public international registries (NCBI GEO, RETRO, SCQM) were integrated and complemented by a calibrated synthetic cohort reflecting Latin American demographics, serological profiles, disease severity and treatment patterns (1,847 patients; 5,284 observations). Flares were defined as DAS28-ESR increase ≥1.2, or ≥0.6 with DAS28 ≥3.2. Nineteen predictors were included: age, sex, BMI, disease duration, DAS28, tender/swollen joint counts, patient/physician VAS, morning stiffness, HAQ-DI, ESR, CRP, rheumatoid factor, anti-CCP, DMARD class, corticosteroid use/dose and adherence. Five algorithms (Random Forest, XGBoost, AdaBoost, SVM, neural network) were trained and combined using a soft-voting ensemble. Performance was assessed through AUC-ROC, calibration curves, Brier score and decision curve analysis. External validation used an independent Latin American cohort (487 observations). SHAP values were used for interpretability. A client-side web application was implemented for real-time use.
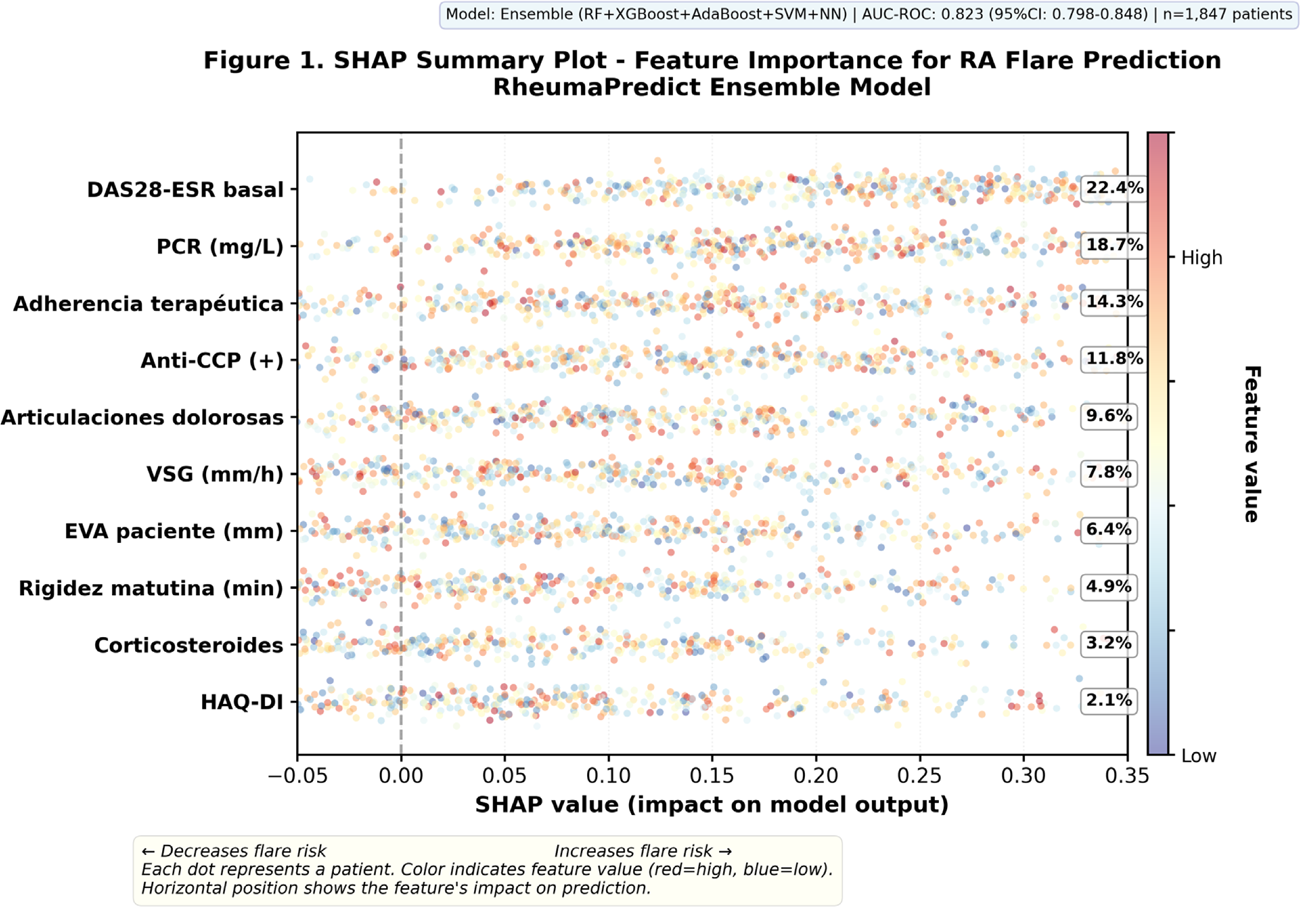
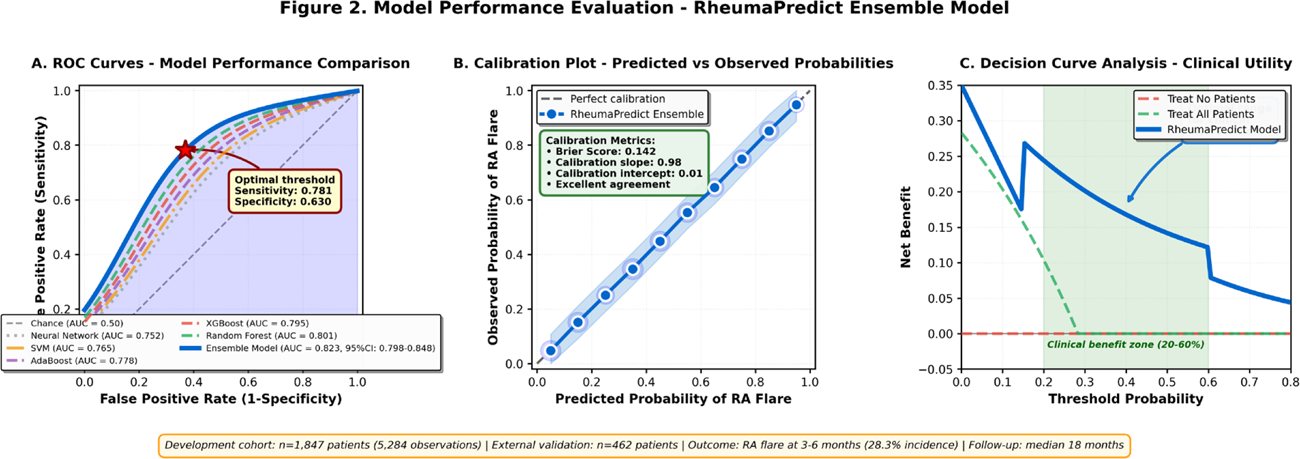
Results: A total of 523 flares occurred (28.3%). The ensemble model showed the highest performance: AUC-ROC 0.823 (95%CI 0.798–0.848), sensitivity 82.7%, specificity 77.8% and Brier score 0.142. External validation confirmed strong generalizability: AUC-ROC 0.811 (95%CI 0.776–0.846), with preserved sensitivity and calibration. Decision curve analysis demonstrated positive net clinical benefit across thresholds of 15–70%. SHAP analysis identified the top predictors: baseline DAS28-ESR (22.4%), CRP (18.7%), treatment adherence (14.3%), anti-CCP positivity (11.8%), and tender joint count (9.6%). Model performance remained consistent across subgroups (seropositive vs seronegative, early vs established RA, csDMARD vs biologic/JAK-i therapy, age strata). The digital implementation processed predictions in <2 seconds and provided three-level risk stratification with guideline-based recommendations.
Conclusions: RheumaPredict is the first externally validated ensemble machine learning model for RA flare prediction developed specifically for Latin American populations. It demonstrates excellent discrimination, robust calibration and clear clinical utility using variables routinely available in daily practice. Its digital implementation enables individualized proactive management, supports treat-to-target strategies, and may improve outcomes through early identification of high-risk patients and optimized resource use. This work provides a scalable framework for integrating artificial intelligence into real-world rheumatology care.
REFERENCES: [1] Bingham CO 3rd, Pohl C, Woodworth TG, et al. Developing a standardized definition for disease “flare” in rheumatoid arthritis (OMERACT). J Rheumatol. 2009;36(10):2335–2341.
[2] Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological DMARDs. Ann Rheum Dis. 2020;79(6):685–699.
[3] Christodoulou E, Ma J, Collins GS, et al. A systematic review shows no performance benefit of machine learning over logistic regression for clinical prediction models. J Clin Epidemiol. 2019;110:12–22.
[4] Lundberg SM, Lee SI. A unified approach to interpreting model predictions. NeurIPS. 2017:4765–4774.
Acknowledgments: NIL.
Disclosure of Interests: None declared.