fetching data ... 
Background: Due to the aging population, the proportion of individuals aged >65 years in the European Union is projected to increase from one-fifth today to nearly one-third by 2050. Consequently, the incidence of elderly-onset rheumatoid arthritis (EORA)—defined as RA diagnosed after the age of 65—is expected to increase substantially. Unlike patients with young-onset rheumatoid arthritis (YORA), EORA is frequently complicated by comorbidities, polypharmacy, and geriatric syndromes such as frailty. In addition, EORA differs from YORA in its immunopathology—such as features of immunosenescence— and is more often seronegative, though findings are conflicting. Although recent evidence indicates that EORA patients can achieve remission rates comparable to YORA patients if a treat-to-target (T2T) management approach is applied, the pharmacotherapeutic needs and adverse event (AE) profile of EORA patients remain poorly understood.
Objectives: Our aim was to determine whether pharmacotherapeutic needs and AE profiles over 2-year follow-up differ between newly diagnosed EORA and YORA patients if a T2T strategy, aiming for low disease activity (LDA), with a fixed medication protocol is applied.
Methods: Data from the Rotterdam Early Arthritis Cohort (tREACH) trial, a multicenter, stratified, single-blinded randomized controlled trial, were used. Patients meeting the 1987 and/or 2010 classification criteria for RA were included and categorized as EORA (onset >65 years; n=98) or YORA (onset 18-65 years; n=327). All patients were managed with a T2T strategy, aiming for LDA (disease activity score [DAS] ≤ 2.4), with a fixed medication protocol. DAS trajectories and treatment alterations were analyzed using multilevel mixed-effect models. Descriptive statistics were applied to evaluate disease modifying antirheumatic drug (DMARD) and glucocorticoid (GC) use, as well as prevalence of difficult-to-treat (D2T) RA, defined as treatment with ≥2 biologic (b)DMARDs with different modes of action and a concomitant reduction in quality of life, during and after 2 years of follow-up. Cox proportional hazard models assessed first bDMARD survival and DMARD-free remission attainment (DFR; no swollen joints and no DMARD for ≥6 months). AEs were prospectively recorded. To account for potential effects of autoantibody status on disease outcomes, a sensitivity analysis was performed in which autoantibody negative EORA and autoantibody negative YORA were compared as well as autoantibody positive EORA and autoantibody positive YORA.
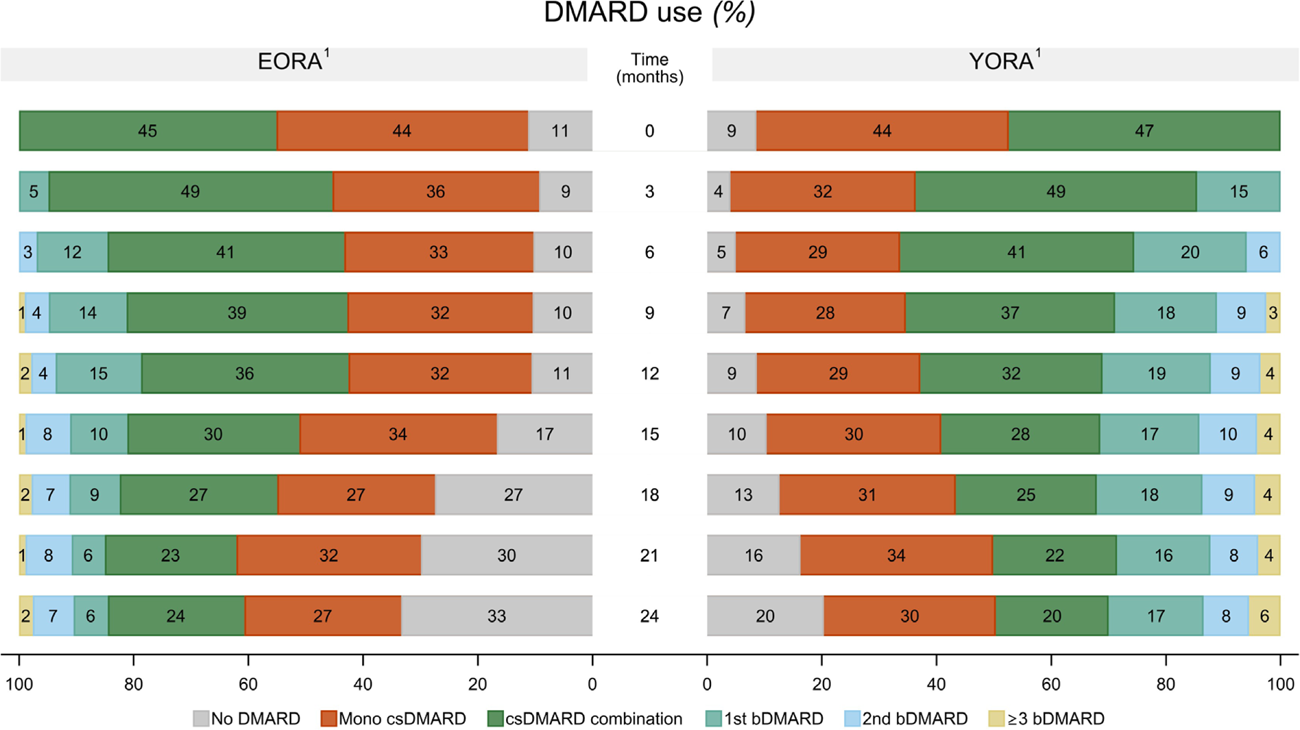
Results: Among the 425 included RA patients, 98 (23%) patients were categorized as EORA (mean age 73 years, standard deviation [SD] 5 years) and 327 (77%) as YORA (mean age 48 years, SD 11 years). EORA patients were more frequently male (50% vs 28%) and had more often ≥1 comorbidity (76% vs 49%). DAS trajectories were similar between groups (mean difference 0.03, 95% confidence interval [CI] -0.13 to 0.18), however EORA patients needed less intensive therapy to achieve LDA (odds ratio [OR] 0.38, 95% CI 0.14 to 0.99) (Figure 1). First bDMARD survival (hazard ratio [HR] 1, 95% CI 0.6 to 1.8) and GC use was comparable, while EORA had a higher probability of achieving DFR (HR 2.2, 95% CI 1.0 to 4.8). At 2 years, D2T RA occurred in 2% of EORA and 6% of YORA patients, a non-significant difference. Bone marrow depression (15% vs. 7%) and elevated creatinine (8% vs. 2%) were significantly more frequent in EORA patients, whereas headache (8% vs. 17%), fatigue (21% vs. 36%), and low mood (6% vs. 17%) were significantly more common in YORA. DMARD switch or dosage adjustment due to AEs did not differ. Sensitivity analysis showed that autoantibody-negative EORA patients needed less intensive therapy (OR 0.31, 95% CI 0.14 to 0.72) and had a higher chance of achieving DFR (HR 3.5, 95% CI 1.3 to 9.4) than autoantibody-negative YORA patients, with reduced DMARD use and similar GC exposure. No differences were observed in all outcomes between autoantibody-positive EORA and autoantibody-positive YORA patients.
Conclusions: A T2T strategy aiming for LDA is feasible and effective in EORA, often requiring less intensive treatment, especially in autoantibody-negative cases. Despite differing AE profiles, overall drug tolerability was comparable between EORA and YORA patients. These findings support implementing T2T strategies in EORA patients whenever clinically applicable.
Medication usage over 2-year follow-up, stratified by RA onset age.
1 EORA includes patients with RA onset after age 65, whereas YORA includes patients with RA onset between ages 18 and 65.
Abbreviations: bDMARD, biologic DMARD; csDMARD, conventional synthetic DMARD; DMARD, disease-modifying antirheumatic drug; EORA, elderly-onset RA; RA, rheumatoid arthritis; and YORA, young-onset RA.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.