fetching data ... 
Background: Rising healthcare expenditures and workforce shortages necessitate the development of alternative strategies to optimise the efficiency of rheumatology care. The recent TeleSpA randomised controlled trial (RCT) demonstrated that patient-initiated follow-up (PIFU, whereby patients only seek care on demand) supported by asynchronous telemedicine (TM) led to a clinically meaningful mean reduction of 25.4% in the number of outpatient visits in patients with stable spondyloarthritis (SpA) compared with usual care (UC), without compromising health outcomes or satisfaction with care [1,2]. To uphold equitability, it is important to investigate whether PIFU/TM is suitable for all patients.
Objectives: To evaluate whether, within pre-specified subgroups of patients with SpA defined by different demographic and clinical characteristics, the effectiveness of PIFU/TM compared with UC is consistent.
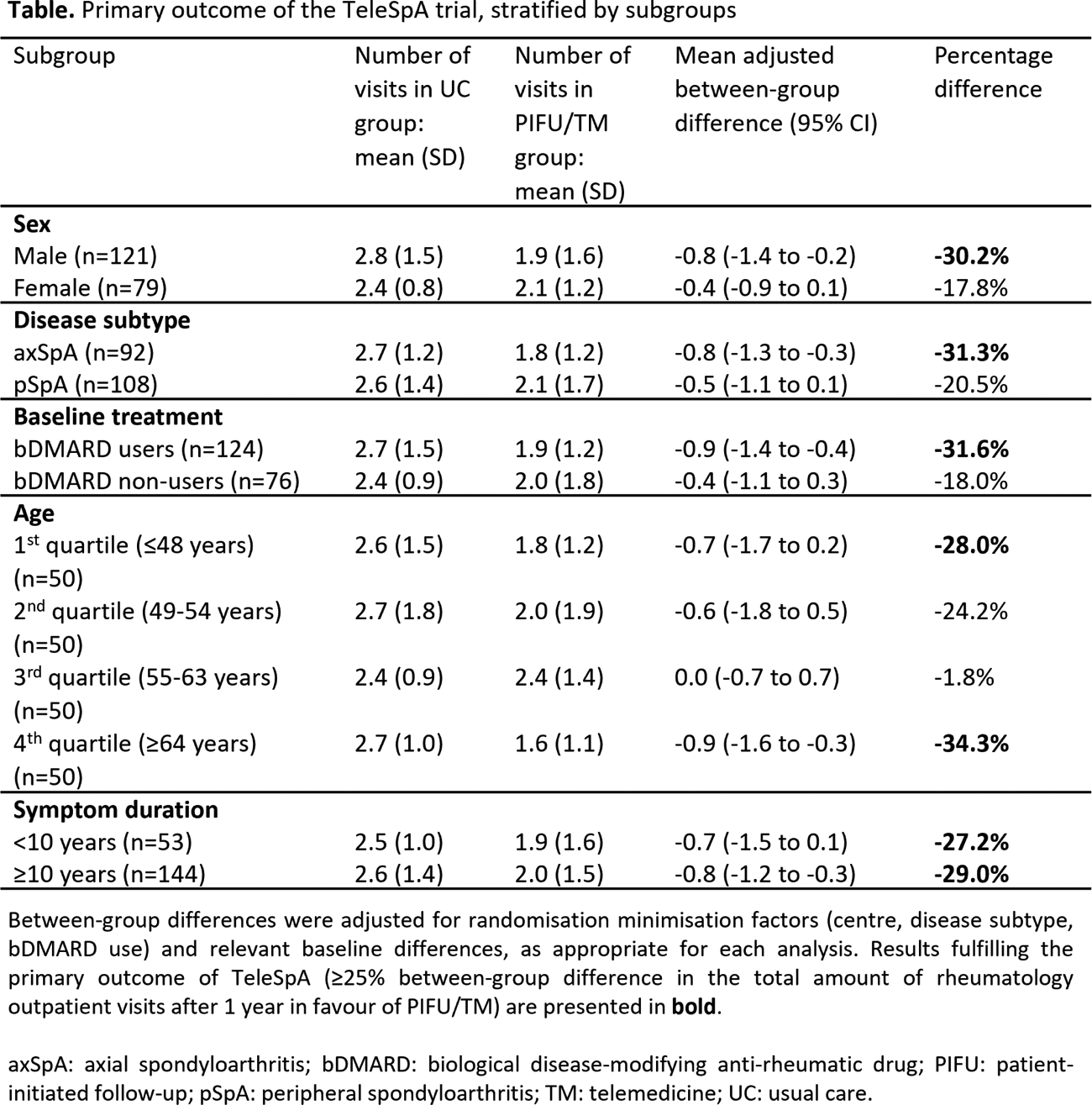
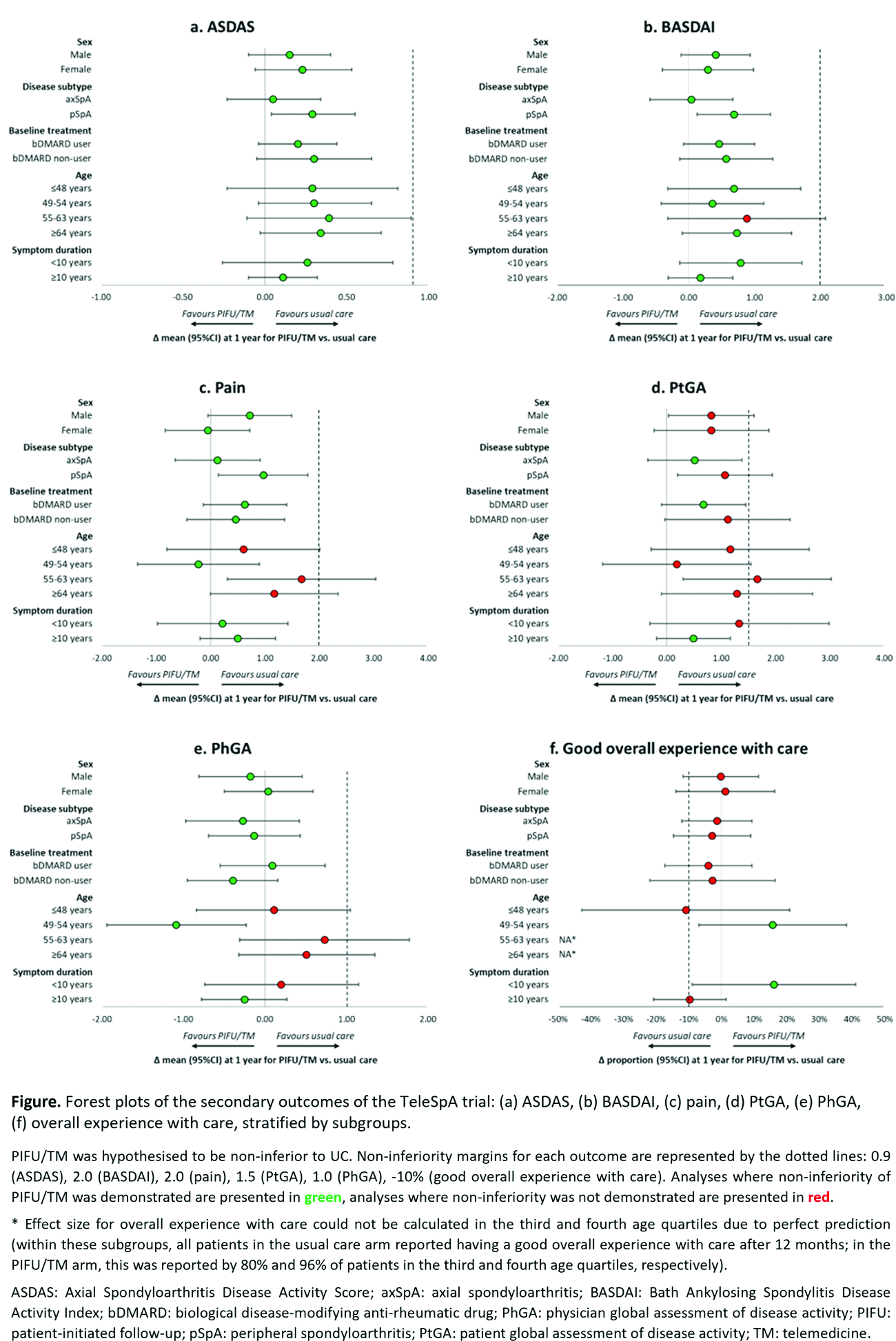
Methods: TeleSpA was a multicentre, pragmatic, open-label RCT (ClinicalTrials.gov identifier: NCT04673825) conducted between 2 December 2020 and 20 June 2022, which included 200 patients with stable SpA randomised 1:1 to PIFU/TM (pre-planned visit after 1 year with asynchronous remote monitoring at 6 months) or UC (pre-planned visit after 1 year with regular visits in-between at discretion of the treating rheumatologist) [1]. In both arms, extra on-demand visits were planned if deemed necessary by the patient. All trial participants were included in this subgroup analysis [3]. Subgroups were formed through stratification by sex (male/female), disease subtype (axial [axSpA]/peripheral [pSpA]), treatment at baseline (biological DMARD [bDMARD] user/non-user), age (by quartiles) and symptom duration (<10 years/≥10 years). The primary outcome in the original trial was a between-group difference ≥25% in the total number of rheumatology outpatient visits after 1 year in favour of PIFU/TM. The secondary outcome was non-inferiority of PIFU/TM compared with UC regarding disease activity (measured with ASDAS, BASDAI, pain [0-10 NRS], patient and physician global assessment of disease activity [PtGA/PhGA, 0-10 NRS]), as well as overall experience with care (% with good experience). In this pre-specified analysis, patients in the PIFU/TM and UC arms within each subgroup were compared. Within subgroups, the primary and secondary outcomes were analysed with AN(C)OVA, with adjustment for randomisation minimisation factors and relevant baseline differences for all outcomes. The present analyses are intended as exploratory, as TeleSpA was not originally powered for subgroup-level effects [3].
Results: In the overall PIFU/TM (n=100) and UC (n=100) arms, respectively, 38% and 41% were female; the mean age was 55.8 (SD 12.3) and 54.2 (SD 11.4) years; and the mean symptom duration was 18.3 (SD 12.4) and 15.8 (SD 8.3) years. In both arms, 46% had axSpA and 54% had pSpA, and 62% used a bDMARD. For the primary outcome, an overall reduction in rheumatology outpatient visits in the PIFU/TM compared with UC arm was observed in all patient subgroups. However, the magnitude of this effect varied (Table 1). When stratified by sex, the primary outcome was only attained among male patients (mean adjusted difference in number of visits -0.8 [95%CI -1.4 to -0.2], 30.2% reduction). Regarding disease subtypes, the primary outcome was attained in patients with axSpA (mean adjusted difference -0.8 [95%CI -1.3 to -0.3], 31.3% reduction) but not in those with pSpA. When considering treatment at baseline, the primary outcome was attained by bDMARD users (mean adjusted difference -0.9 [95%CI -1.4 to -0.4], 31.6% reduction) but not by non-users. Across age quartiles, the primary outcome was attained only in the first quartile (≤48 years: mean adjusted difference -0.7 [95%CI -1.7 to 0.2], 28.0% reduction) and fourth quartile (≥64 years: mean adjusted difference -0.9 [95%CI -1.6 to -0.3], 34.3% reduction). A notably low between-group difference was observed in the third age quartile (55-63 years: 1.8% reduction). Finally, when stratified by symptom duration, the primary outcome was attained both in patients with symptoms for <10 years (mean adjusted difference -0.7 [95%CI -1.5 to 0.1], 27.2% reduction) and those with symptoms for ≥10 years (mean adjusted difference -0.8 [95%CI -1.2 to -0.3], 29.0% reduction). Regarding the secondary outcomes, non-inferiority was demonstrated for ASDAS in all subgroups, and for BASDAI in all but one subgroup (Figure 1). Non-inferiority for pain and PhGA was demonstrated in both sexes, both SpA subtypes and bDMARD users and non-users, as well as within the second age quartile and patients with a symptom duration ≥10 years. In patients in the first, third and fourth age quartiles and patients with a symptom duration <10 years, non-inferiority was not demonstrated for multiple health outcomes, albeit with largely similar effect sizes in comparison with the subgroups in which non-inferiority was demonstrated. Non-inferiority for PtGA and overall experience with care was only sporadically demonstrated.
Conclusions: Meaningful reductions in rheumatology outpatient visits were attained through PIFU/TM compared with UC in patients with stable SpA, particularly in certain clinical subgroups: males, axSpA subtype, bDMARD users, patients in the youngest and oldest age quartiles, and patients across all symptom durations. Non-inferiority regarding health outcomes was not universally demonstrated, plausibly due to insufficient statistical power in the individual subgroups. Broader knowledge on the suitability of PIFU/TM across subgroups may enable more patient-centred care delivery.
REFERENCES: [1] Hermans K. et al. Lancet Rheumatol 2024;6(12):e848-59, doi: 10.1016/S2665-9913(24)00229-7.
[2] Smits M.L. et al. Rheumatology (Oxford) 2025;64(5):2631-9, doi: 10.1093/rheumatology/keae650.
[3] Hermans K. et al. BMJ Open 2023;e067445, doi: 10.1136/bmjopen-2022-067445.
Acknowledgments: NIL.
Disclosure of Interests: Marius L. Smits Novartis, Hosna Salmani: None declared, Annelies Boonen Johnson & Johnson, AbbVie, Pfizer, UCB, AbbVie, Eli Lilly, Kasper Hermans UCB, Harald E. Vonkeman AstraZeneca, Eli Lilly, Pfizer, Alfasigma, AbbVie, Novartis, Pfizer, UCB, Johnson & Johnson, Alfasigma, Galapagos, Boehringer Ingelheim, Astrid van Tubergen Pfizer, Novartis, AbbVie, Novartis, Johnson & Johnson, UCB, Novartis, UCB, AbbVie, Casper Webers Novartis, AbbVie.