fetching data ... 
Background: Upadacitinib, an oral JAK1 inhibitor, has demonstrated efficacy and safety in patients with active axial spondyloarthritis (axSpA), including both radiographic (r-axSpA) and non-radiographic axSpA (nr-axSpA) [1]. However, there is limited evidence regarding maintenance of remission after discontinuation of upadacitinib therapy in patients who had achieved an initial response.
Objectives: To assess the maintenance of disease control following the withdrawal and subsequent retreatment with upadacitinib in patients with axSpA who experience a disease flare after achieving clinical remission.
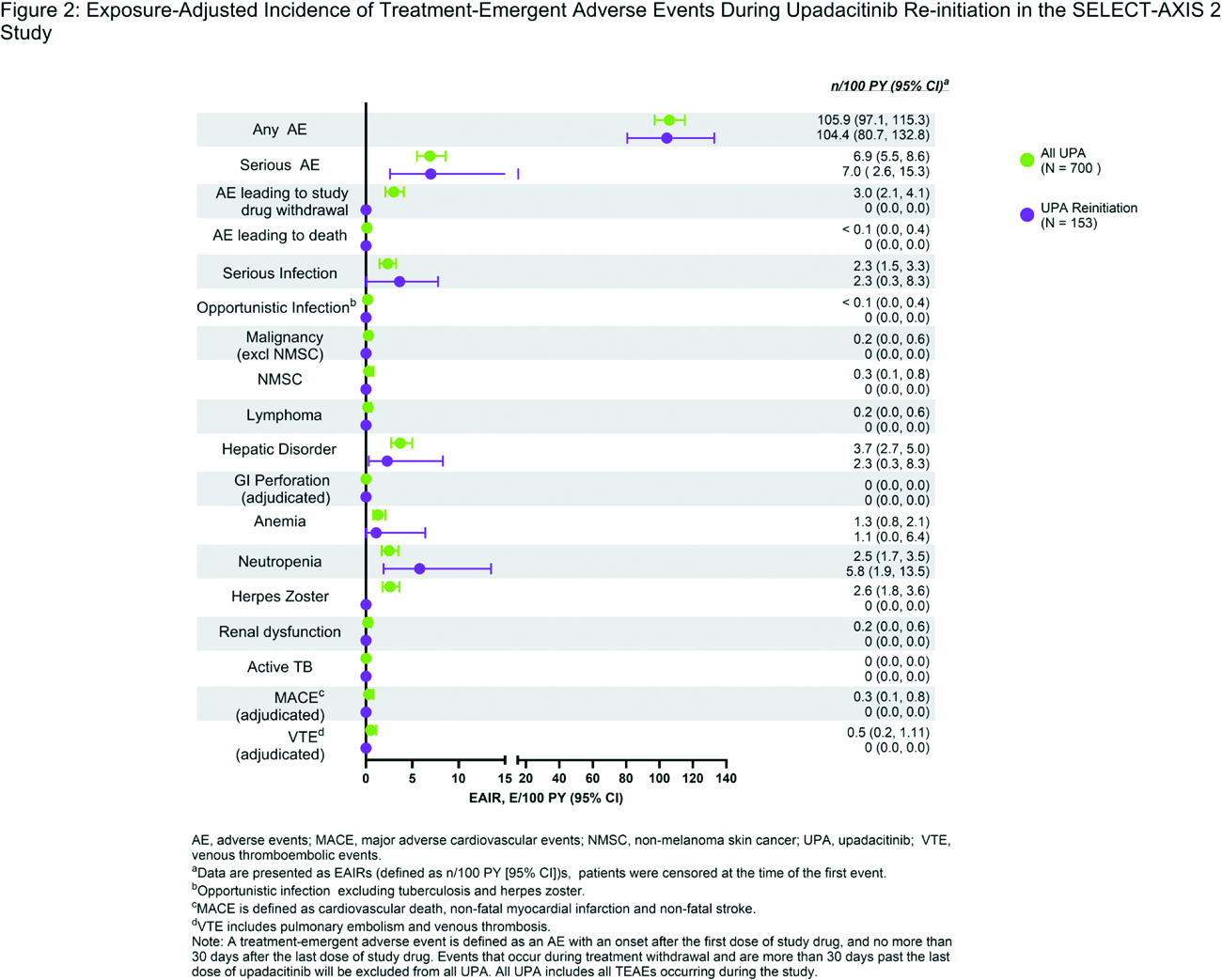
Methods: SELECT-AXIS 2 (NCT04169373) is a phase 3, placebo-controlled, double-blind trial involving patients with axSpA (fulfilling modified New York criteria) who had an inadequate response or were intolerant to biologic DMARDs (bDMARD-IR) and patients with nr-axSpA. Patients received either upadacitinib 15 mg or placebo. At week 104, those in clinical remission (defined by ASDAS < 2.1 at week 88 and ASDAS < 1.3 at week 104) entered an open label treatment withdrawal period. In the event of a disease flare (defined by ASDAS (CRP) ≥ 2.1 at two visits at least two weeks apart, or ASDAS > 3.5 at one visit) during the withdrawal period, patients re-initiated upadacitinib 15 mg daily for 24 weeks. Outcomes assessed included the median time to flare during the withdrawal period and the proportions of patients achieving ASDAS low disease activity (LDA; < 2.1) and inactive disease (ID; < 1.3) scores during the retreatment period after a disease flare. Patients who did not experience a flare were monitored until week 152. Data are reported as observed without imputation of missing values. Safety data were summarized using exposure-adjusted incidence rates (EAIRs per 100 patient-years) for patients who received at least one dose of upadacitinib during the re-initiation phase, as well as for those who received the drug throughout the entire study period.
Results: Out of 734 patients participating in the SELECT-AXIS 2 study, 194 patients (26.4%) were in remission at week 104 and were included in this analysis (r-axSpA bDMARD-IR, n = 114; nr-axSpA, n = 80). Following 48 weeks of withdrawal of upadacitinib treatment, 22.2% of patients maintained pre-defined clinical remission, while the median time to flare was: 3.1 months (2.8 months for r-axSpA bDMARD-IR, and 5.0 months for nr-axSpA). ( Figure 1A ). Upon re-initiation of upadacitinib therapy, 72.2% (n/N, 96/133) of patients achieved ASDAS LDA (< 2.1) by week 4 and 88.9% (104/117) achieved ASDAS LDA (< 2.1) by week 24 ( Figure 1B ). Additionally, ASDAS ID (< 1.3) was achieved by 35.3% (47/133) of patients by week 4 and by 48.7% (57/117) by week 24 after re-treatment ( Figure 1C ). Upadacitinib was generally well-tolerated during re-treatment and in the long-term, with no new safety concerns or significant risks identified. The safety profile remained consistent with previous reports 1 , supporting the continued use of upadacitinib 15 mg once daily in patients with active axSpA. ( Figure 2 ).
Conclusions: Continuous treatment with upadacitinib is necessary for maintaining disease control in axSpA. However, only about one-fourth of patients may achieve long-term drug-free remission. In patients who experience a disease flare after discontinuation, the majority regain at least ASDAS LDA within 24 weeks of therapy reinitiation. These findings are crucial in guiding treatment decisions when therapy interruptions are necessary.

REFERENCES: [1] Burmester GR et al. Adv Ther . 2025; 10:5215-37.
Acknowledgments: NIL.
Disclosure of Interests: Atul Deodhar has received honoraria or consultation fees from AbbVie, BMS, Janssen, Lilly, Novartis, Pfizer, and UCB Pharma, grant/research support from AbbVie, BMS, Celgene, Lilly, MoonLake, Novartis, Pfizer, and UCB Pharma, Mitsumasa Kishimoto has received consulting fees and/or honoraria from AbbVie, Amgen, Asahi-Kasei Pharma, Ayumi Pharma, BMS, Chugai, Daiichi Sankyo, Eisai, Gilead, Janssen, Lilly, Novartis, Ono Pharma, Pfizer, Tanabe-Mitsubishi, and UCB Pharma, Denis Poddubnyy has received speaking fees AbbVie, Biocad, BMS, Galapagos, Gilead, GSK, Janssen, Lilly, MSD, Medscape, MoonLake, Novartis, Peervoice, Pfizer, Roche, Samsung Bioepis, and UCB Pharma, consulting fees and/or honoraria AbbVie, Biocad, BMS, Galapagos, Gilead, GSK, Janssen, Lilly, MSD, Medscape, MoonLake, Novartis, Peervoice, Pfizer, Roche, Samsung Bioepis, and UCB Pharma, research support from AbbVie, Lilly, MSD, Novartis, and Pfizer, Walter P Maksymowych has received speaking fees from AbbVie, BMS, Celgene, Galapagos, Gilead, Janssen, Lilly, Medscape, Novartis, Peervoice, Pfizer, and UCB Pharma, royalties or licences from Augurex for the 14-3-3eta diagnostic biomarker and is Chief Medical Officer at CARE Arthritis Limited, consulting fees and/or honoraria fees from AbbVie, BMS, Celgene, Galapagos, Gilead, Janssen, Lilly, Medscape, Novartis, Peervoice, Pfizer, and UCB Pharma, grant/research support from AbbVie, Novartis, Pfizer, and UCB Pharma, Ivan Lagunes may hold stock or stock options at AbbVie, employee of AbbVie, Koji Kato may hold stock or stock options at AbbVie, employee of AbbVie, Bhumik Parikh may hold stock or stock options at AbbVie, employee of AbbVie, Kyle Carter may hold stock or stock options at AbbVie, employee of Abbvie, Charles Phillips may hold stock or stock options at AbbVie, employee of AbbVie, Xenofon Baraliakos has received speakers’ bureau fees from AbbVie, BMS, Celgene, Chugai, Merck, Novartis, Pfizer, and UCB Pharma, consulting fees from AbbVie, BMS, Chugai, MSD, Novartis, Pfizer, and UCB Pharma and is an editorial board member of the Annals of Rheumatic Diseases, is the ASAS President and is the EULAR President-elect, grant/research support from AbbVie and Novartis.