fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a systemic autoimmune disease primarily affecting young women [1]. An extensive and robust body of data has demonstrated the existence of an accelerated atherosclerosis phenomenon in SLE patients [2]. Despite this increased risk profile, optimal cardiovascular risk prediction and prevention strategies remain yet to be defined [3].
Objectives: This study aimed to identify distinct cardiovascular risk phenotypes in SLE using an unsupervised cluster analysis, and to compare the risk of incident cardiovascular events and subclinical atherosclerosis progression in the identified subgroups.
Methods: Consecutive SLE patients who underwent a comprehensive cardiovascular risk assessment at the French National Referral Center for SLE between 2014 and 2024 were retrospectively included. An unsupervised analysis was performed using a hierarchical clustering algorithm on clinical (age, sex, SLE duration, antiphospholipid syndrome [APS], hypertension, diabetes, body-mass index [BMI], smoking), biological (estimated glomerular filtration rate and fasting lipid profile including total cholesterol [TC], high-density lipoprotein [HDL], low-density lipoprotein [LDL] and triglycerides [TG]) and imaging variables (coronary artery calcium [CAC] score, epicardial adipose tissue [EAT] volume). Incident atherosclerotic cardiovascular disease (ASCVD) events, follow-up CAC scores and annualized CAC progression rates [4] were compared across the identified clusters.
Results: A total of 226 patients were included (91% females, 45±13 years). SLE duration was 13 ± 9 years. Prior organ involvement included articular manifestations in 202 patients (89%), skin manifestations in 151 patients (67%), lupus nephritis in 76 patients (34%) and pleural or pericardial effusions in 50 patients (22%). APS was present in 23 patients (10%). A total of 213 patients (94%) were on hydroxychloroquine, 151 (67%) on corticosteroids, and 115 (51%) were receiving or had received conventional synthetic disease-modifying antirheumatic drugs.
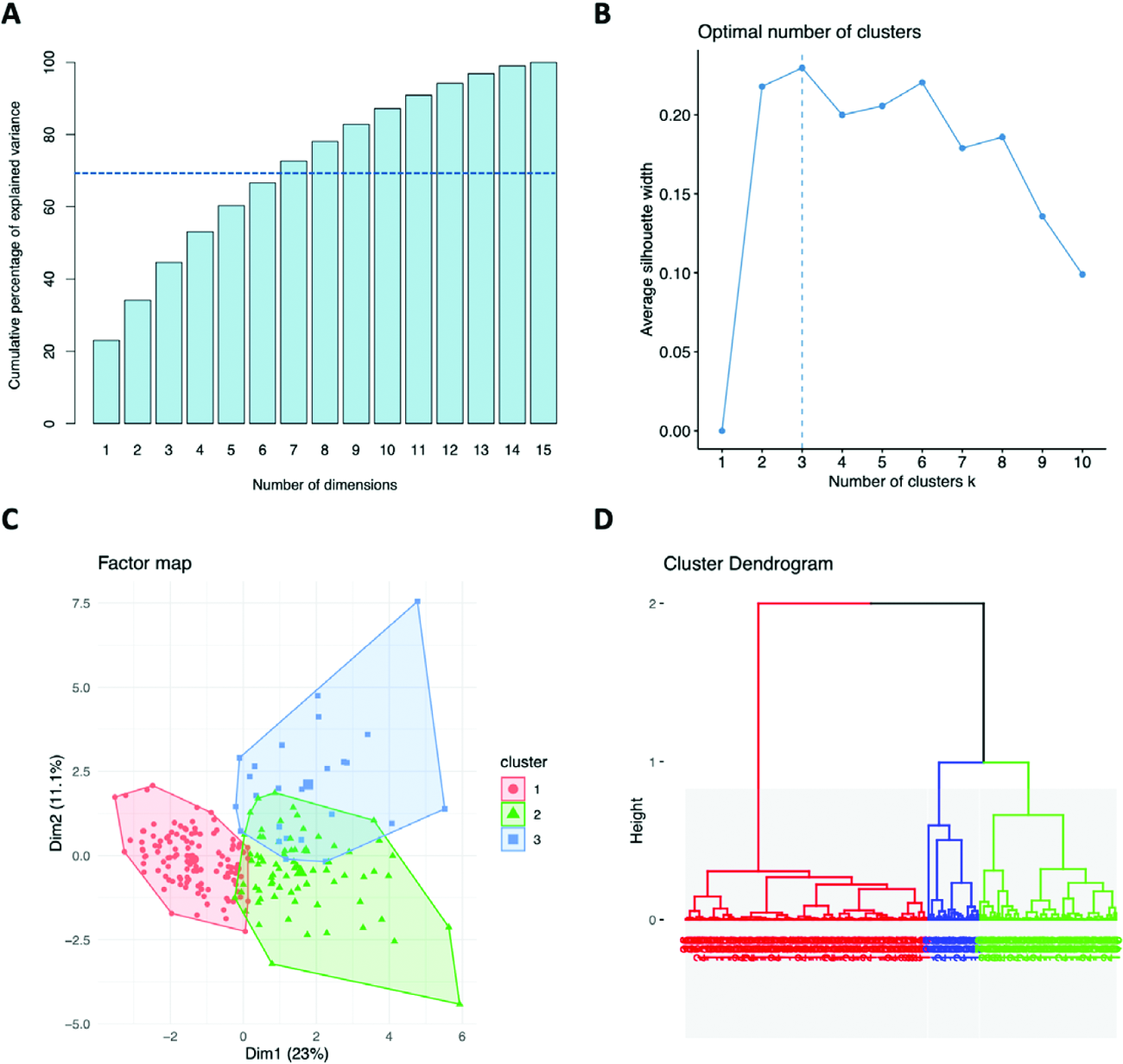
Three clusters were identified (Figure 1).
Cluster 1 (N=123) included young (37±9 years) female patients (98%) with few traditional cardiovascular risk factors (hypertension 11%, smoking 20%, BMI 23±4 kg/m 2 , diabetes 1%, LDL 0.9±0.3 g/L, TG 0.7±0.3 g/L, eGFR 101±16 mL/min/1.73m 2 , APS 2%). SLE duration was 10±7 years and corticosteroids cumulative exposure was 14±12 g. Mean CAC score was 5±23. EATi volume was 43±16 mL/m 2 .
Cluster 2 (N=78) included older (54±9 years) female patients (96%) with significant cardiovascular risk factors (hypertension 44%, smoking 35%, BMI 28±7 kg/m 2 , diabetes 0%, LDL 1.3±0.4 g/L, TG 0.9±0.4 g/L, eGFR 77±23 mL/min/1.73m 2 , APS 21%). SLE duration was longer (19±9 years) and corticosteroids cumulative exposure was high (23±15 g). Mean CAC score was 42±123. EATi volume was increased at 81±30 mL/m 2 in this cluster.
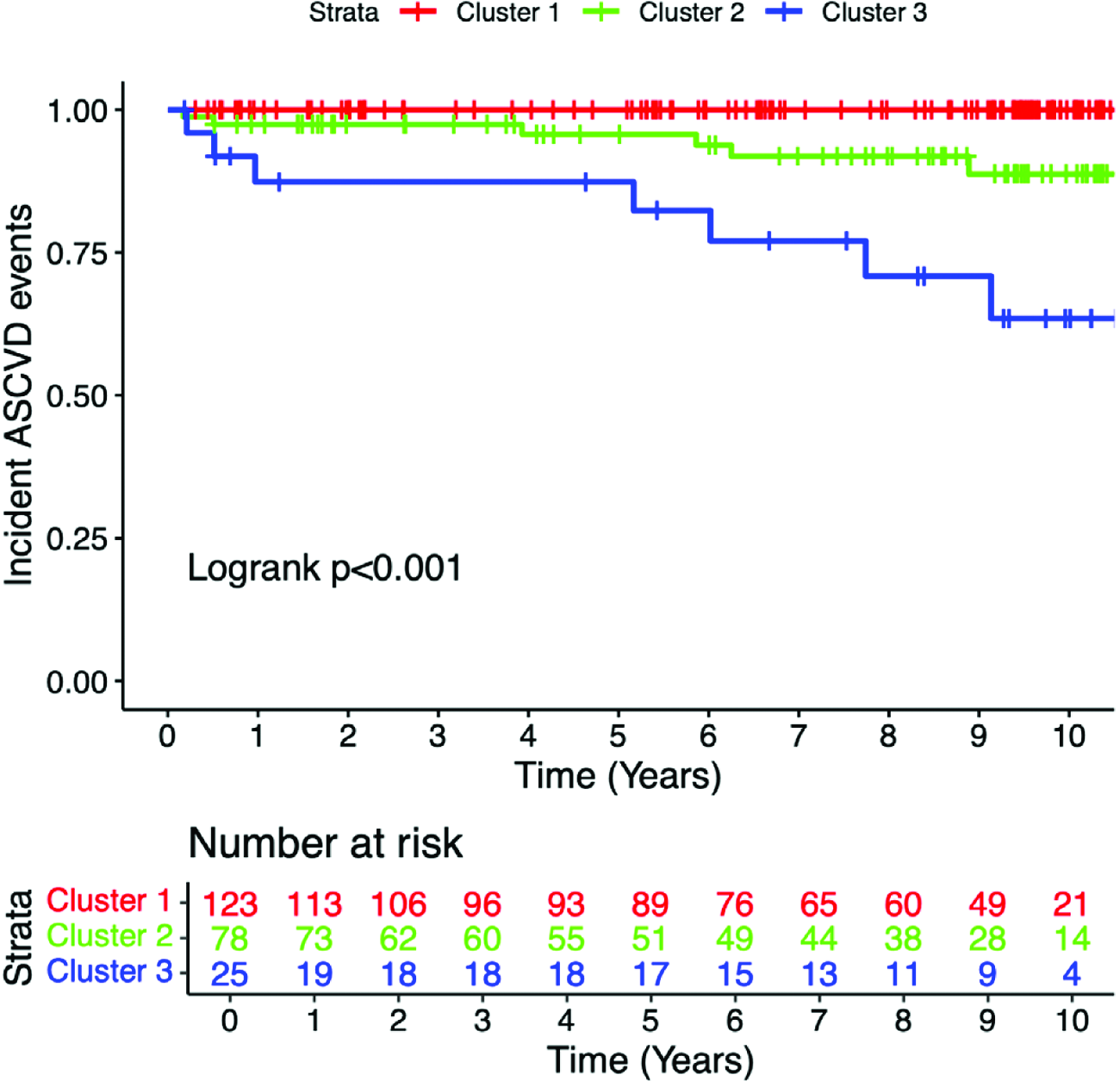
Cluster 3 (N=25) included middle-aged (51±13 years) patients with an increased male prevalence (60%) and frequent cardiovascular risk factors (hypertension 52%, smoking 44%, BMI 28±5 kg/m 2 , diabetes 48%, LDL 1±0.3 g/L, TG 1.4±0.8 g/L, eGFR 92±17 mL/min/1.73m 2 , APS 16%). SLE duration was 12±9 years and corticosteroids cumulative exposure was 15±12 g. Mean CAC score of 112±356. EATi volume was the highest of all three cluster (103±47 mL/m 2 ). After a median follow-up of 8 [4–10] years, no events were observed in cluster 1 (0%), compared with 6 (8%) in cluster 2 and 7 (28%) in cluster 3. On survival analysis, the risk of incident ASCVD events significantly differed between cluster (Log-rank P <0.001, Figure 2). A subset of 95 patients had a follow-up cardiac CT after a mean follow-up duration of 4±4 years. Follow-up CAC scores significantly differed across the three clusters (cluster 1: 14±52, cluster 2: 133±303, cluster 3: 293±571, P =0.004) and so did CAC progression rates (cluster 1: 0.1±0.1, cluster 2: 0.6±1, cluster 3: 0.7±1.2, P =0.006). A post-clustering decision tree identified (i) age ≥ 48 years-old, (ii) diabetes mellitus, and (iii) epicardial adipose tissue volume ≥ 71 ml/m 2 as key determinants of cluster membership with a sensitivity of 73% and a specificity of 81%.
Conclusions: Cardiovascular risk in SLE comprises three subgroups with distinct phenotypes, risks of incident events and subclinical atherosclerosis progression. These findings identify cardiometabolic risk factors as key drivers of SLE-related atherosclerosis, supporting the evaluation of GLP-1 receptor agonists to mitigate cardiovascular risk in SLE[5,6].
Cluster analysis.
A. Cumulative percentage of explained variance (cutoff 70%)
B. Silhouette score.
C. Factor map.
D. Cluster dendrogram.
Incident ASCVD Kaplan-Meier survival curve according to clusters.
REFERENCES: [1] Hoi A, Igel T, Mok CC, et al. Systemic lupus erythematosus. The Lancet . 2024;403:2326–38. doi: 10.1016/S0140-6736(24)00398-2.
[2] Conrad N, Verbeke G, Molenberghs G, et al. Autoimmune diseases and cardiovascular risk: a population-based study on 19 autoimmune diseases and 12 cardiovascular diseases in 22 million individuals in the UK. The Lancet . 2022;400:733–43. doi: 10.1016/S0140-6736(22)01349-6.
[3] Drosos GC, Vedder D, Houben E, et al. EULAR recommendations for cardiovascular risk management in rheumatic and musculoskeletal diseases, including systemic lupus erythematosus and antiphospholipid syndrome. Ann Rheum Dis . 2022;81:768–79. doi: 10.1136/annrheumdis-2021-221733.
[4] Hokanson JE, MacKenzie T, Kinney G, et al. Evaluating Changes in Coronary Artery Calcium: An Analytic Method That Accounts for Interscan Variability. American Journal of Roentgenology . 2004;182:1327–32. doi: 10.2214/ajr.182.5.1821327.
[5] Iacobellis G. Epicardial adipose tissue in contemporary cardiology. Nat Rev Cardiol . 2022;19:593–606. doi: 10.1038/s41569-022-00679-9.
[6] Kyriazi N, Vassilakis KD, Bakiri A, et al. Antiobesity medications in rheumatology. Quo vadis? Annals of the Rheumatic Diseases . 2025;S0003496725043122. doi: 10.1016/j.ard.2025.08.013.
Acknowledgments: NIL.
Disclosure of Interests: Lévi-Dan Azoulay: None declared, Nadjia Kachenoura: None declared, Samia Boussouar: None declared, Etienne Charpentier: None declared, Nicoletta Pasi: None declared, Lan-Anh Nguyen: None declared, Thomas Broussaud: None declared, Alain Giron: None declared, Jonas Leite: None declared, Nassim Ait-Abdallah: None declared, Micheline Pha: None declared, Miguel Hié: None declared, Alexis Mathian A.M. participated in advisory board related to lupus for AstraZeneca; received payment for expert testimony for GSK; received support for attending meetings and/or travel from AstraZeneca, GSK, Novartis and Otsuka; received consulting fees, speaking fees and honoraria from AstraZeneca, GSK, Novartis and Otsuka., Marc Pineton de Chambrun: None declared, Matthias Papo: None declared, Fleur Cohen: None declared, Julien Haroche: None declared, Alban Redheuil: None declared, Zahir Amoura Z.A. reports a relationship with GSK, AstraZeneca, Roche, Novartis, Amgen, Kezar that includes consulting or advisory and funding grants.