fetching data ... 
Background: In patients with rheumatic musculoskeletal diseases (RMDs), the prevalence of sexual dysfunction (SD) is increased; however, this aspect is rarely explored in clinical practice [1]. There is no specialty that assumes responsibility for this domain, which may lead to confusion among both patients and healthcare providers regarding when and with whom it should be discussed [2]. Approximately 40% of women expect healthcare professionals to initiate the conversation, whereas one of the main barriers for physicians is not feeling responsible for this issue and expecting the patient to bring it up [3].
Objectives: Describe the prevalence of where sexual health counselling is provided in patients with RMD: primary care or rheumatologist, and to describe the prevalence of SD according to whom they received the sexual counselling from.
Methods: We conducted a cross-sectional study in adult women (>18 years) with at least one rheumatic disease at the outpatient rheumatology clinic at “Hospital Universitario Dr. José Eleuterio González”. To evaluate the communication, we asked whether at any point a primary care physician or a rheumatologist had discussed sexual health with them. The variable “ Communication ” was categorized into three groups: no physician explored sexual health, only one physician (either primary care or rheumatologist) explored it, or both physicians explored it. Sociodemographic and clinical variables were obtained from medical records.
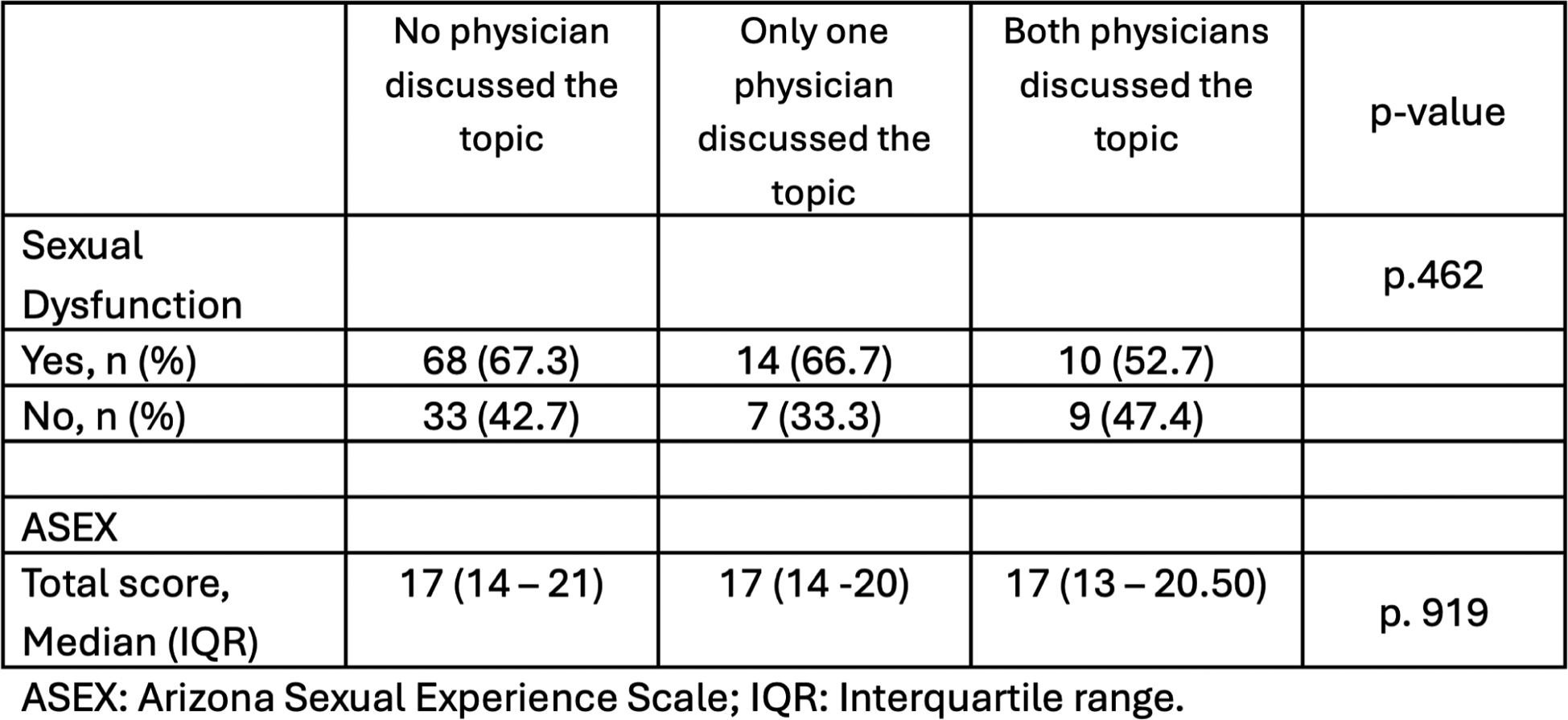
Additionally, a sub-analysis was performed in those patients with an active sexual life. The Arizona sexual experience scale questionnaire (ASEX) was administered to evaluate sexual function. SD was defined as a total score ≥19 points, at least one item with ≥5 points, or two items with ≥4 points.
Categorical variables were reported as frequencies and percentages and compared using the Chi-square test. Normality of continuous variables was assessed with the Shapiro–Wilk test, and group differences were evaluated with the Kruskal–Wallis test.
Results: A total of 243 participants were included. The median age was 47 years (IQR 35–54), and the median disease duration was 4 years (IQR 1–9). Most participants were women, 235 (96.7%), and 146 (60.1%) were in a relationship. The most frequent occupation was homemaker, 134 (55.1%), and approximately half had a low educational level, 128 (52.7%). The majority had children, 180 (74.1%), and among women, 141 (58.8%) were premenopausal (Table 1).
The most common primary diagnosis was rheumatoid arthritis, present in 106 patients (43.6%), followed by systemic lupus erythematosus in 59 (24.3%), osteoarthritis in 18 cases (7.4%), fibromyalgia in 20 (8.2%), inflammatory myopathies in 13 (5.3%), Sjögren’s syndrome in 9 (3.7%), systemic sclerosis in 10 (4.1%), spondyloarthritis in 3 (1.2%), and psoriatic disease in 5 patients (2.1%).
Among the 243 participants, 180 (74.1%) reported that no physician had discussed sexual health, whereas 63 (25.9%) indicated that at least one of their physicians had done so. Within this group, in 26 (41.3%) only the primary care physician discussed the topic, in 11 (17.5%), only the rheumatologist, and in another 26 (41.3%) both physicians did.
No significant differences were found in gender (p = 0.569), marital status (p = 0.776), educational level (p = 0.088), or antidepressant use (p = 0.337). However, differences were found in occupation ( p =.039 ) and menopausal status ( p = 0.019 ).
Of the initial 243 participants, 141 (58.0%) reported being sexually active and were included in the sub-analysis (Table 2). The prevalence of sexual dysfunction in this group was 92 patients (65.2%). No significant differences were observed in the prevalence of sexual dysfunction across the three groups of communication (p =.462). The median ASEX total score was 17 (IQR 14–21), with no differences between groups (p =.919).
Conclusions: Communication about sexual health was infrequent; only one in four patients reported that the topic had been discussed by any physician. In patients who reported that sexual health had been discussed, no significant differences were observed in the prevalence or the severity of SD. Significant differences were noted in premenopausal women and those who were employed. This may reflect a bias among physicians regarding whom to approach, based on the assumption that sexual activity declines in postmenopausal women; however, studies have shown that up to 60% of postmenopausal women remain sexually active (2). Another possibility is that some groups may be more willing to discuss the topic.
These data suggest that communication is limited and likely not effective. Further exploration of the barriers that hinder this communication is needed, along with expanding education for healthcare providers on the management of sexual health.
Table 1. Sociodemographic characteristics by group of communication.
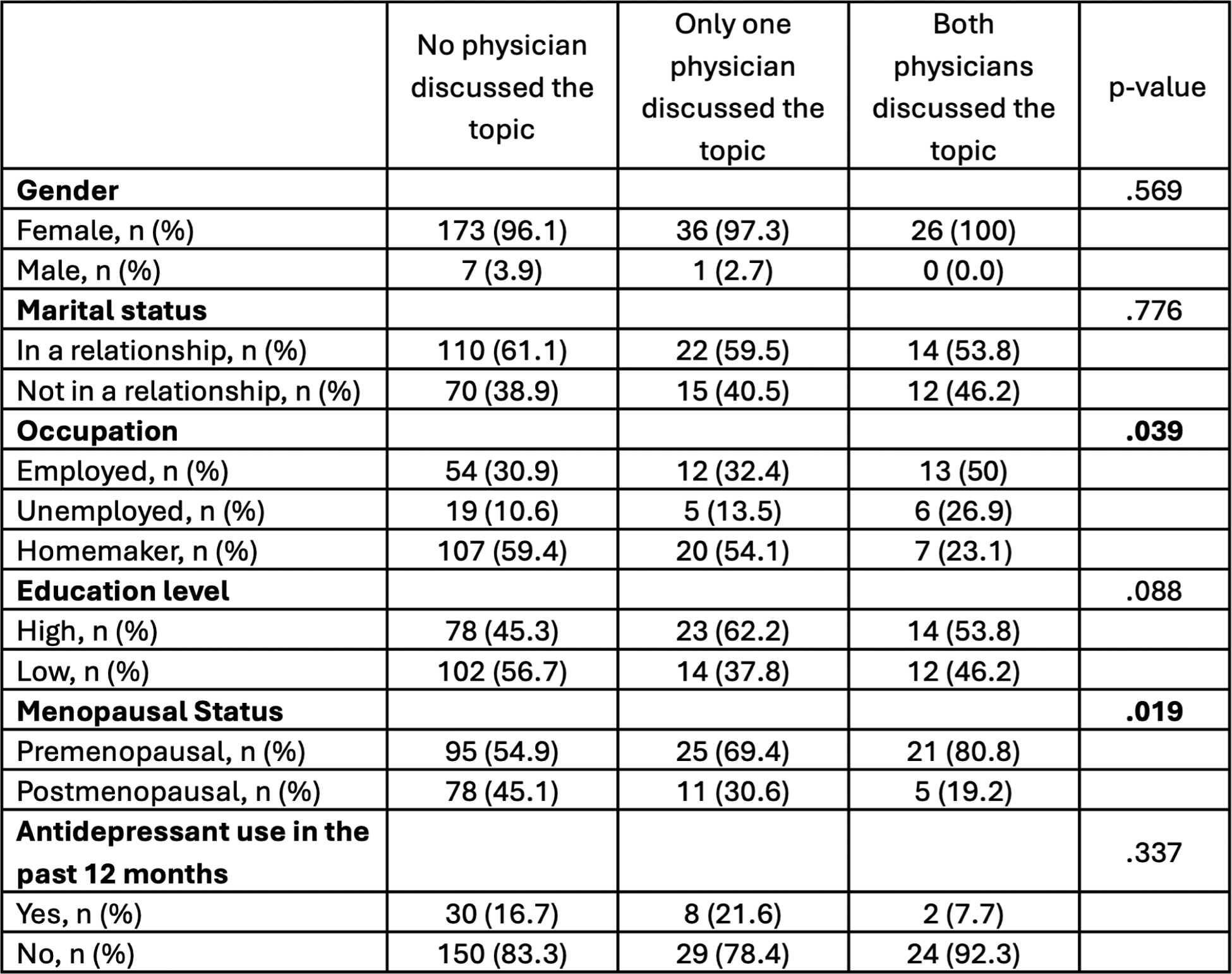
Table 2. Subanalysis of sexual dysfunction stratified by level of communication.
REFERENCES: [1] Østensen M. Sexual and reproductive health in rheumatic disease. Nature Reviews Rheumatology . 2017;13(8):485–93.
[2] Komlenac N, Hochleitner M. Predictors for Low Frequencies of Patient-Physician Conversations Concerning Sexual Health at an Austrian University Hospital. Sexual Medicine . 2020;8(1):100–6.
[3] Kingsberg SA, Schaffir J, Faught BM, Pinkerton JV, Parish SJ, Iglesia CB, et al. Female Sexual Health: Barriers to Optimal Outcomes and a Roadmap for Improved Patient–Clinician Communications. Journal of Women’s Health. 2019;28(4):432–43.
Acknowledgments: NIL.
Disclosure of Interests: None declared.