fetching data ... 
Background: In the absence of biomarkers predicting response to a specific therapy, the choice of second biologic is based mostly on habit and availability of an alternative agent. Traditionally, a second anti-TNF was the preferred option, but recent registry data point to better responses and retention if a drug with a different mode of action is prescribed.
Objectives: Assess the long-term retention of abatacept (ABA) and TNFi following first biologic (b)DMARD inadequate response in RHUMADATA® registry patients (pts) with RA.
Methods: Data from RHUMADATA® pts with RA prescribed either ABA or TNFi as the second bDMARD after 1 January 2006 were analysed. Pts were followed until treatment discontinuation or 9 January 2017 cut-off. Pt characteristics were compared using descriptive statistics, bDMARD discontinuation rates using Kaplan-Meier methods, and proportional hazard models were used to identify predictors of treatment discontinuation.
Results: Data for 92 and 194 pts prescribed ABA or a TNFi, respectively, as second-line treatment were extracted. No clinically significant differences in baseline characteristics were noted between treatment groups. Most pts were women (76.2%), average age (SD) was 45.1 (13.3) years at diagnosis and disease duration 10.8 (9.0) years. Most pts were stopping an anti-TNF agent: 97% of those who were switched to ABA and 83% of those who were prescribed a second anti-TNF. Overall, 77.6% of pts stopped their first bDMARD after >6 months of treatment (secondary failure). Significant differences in retention between ABA and TNFi groups (log-rank p=0.0002) were observed (Table, Figure). Results remained unchanged for pts treated with TNFi only in first line, and primary/secondary failure of the first bDMARD did not affect sustainability of the second agent. Lack of efficacy (57.7%) and AEs (16.5%) were the most commonly cited reasons for treatment discontinuation.
Table 1. First bDMARD failure and retention characteristics of the second bDMARD 1% survival (standard error of % survival).
Second bDMARD TNFi Abatacept First bDMARD Failed Failure type All Failure type All Primary Secondary Primary Secondary TNF inhibitor, n, % 41, 25.5% 120, 74.5% 161, 100% 17, 19.1% 72, 80.9% 89, 100% Other mode of action 6, 18.2% 27, 81.8% 33, 100% 0, 0% 3, 100% 3, 100% Total 47, 24.2% 147, 75.8% 194, 100% 17, 18.5% 75, 81.5% 92, 100% Second bDMARD Retention Probability at1: 6 Months 64.68% (3.45%) 83.51% (3.89%) 12 Months 50.54% (3.61%) 76.73% (4.45%) 24 Months 39.77% (3.59%) 59.97% (5.29%) 60 Months 22.26% (3.53%) 36.95% (6.17%) 96 Months 13.22% (3.62%) 30.66% (6.61%) Biologic Retention Time (years) Mean, mean (SE) 2.71 (0.25) 3.33 (0.26) Lower Quartile (95% CI) 0.36 (0.28–0.44) 1.02 (0.49–1.29) Median (95% CI) 1.08 (0.71–1.60) 3.17 (1.92–4.78) Upper Quartile (95% CI) 4.26 (3.25–6.64) ++ (5.24-++)
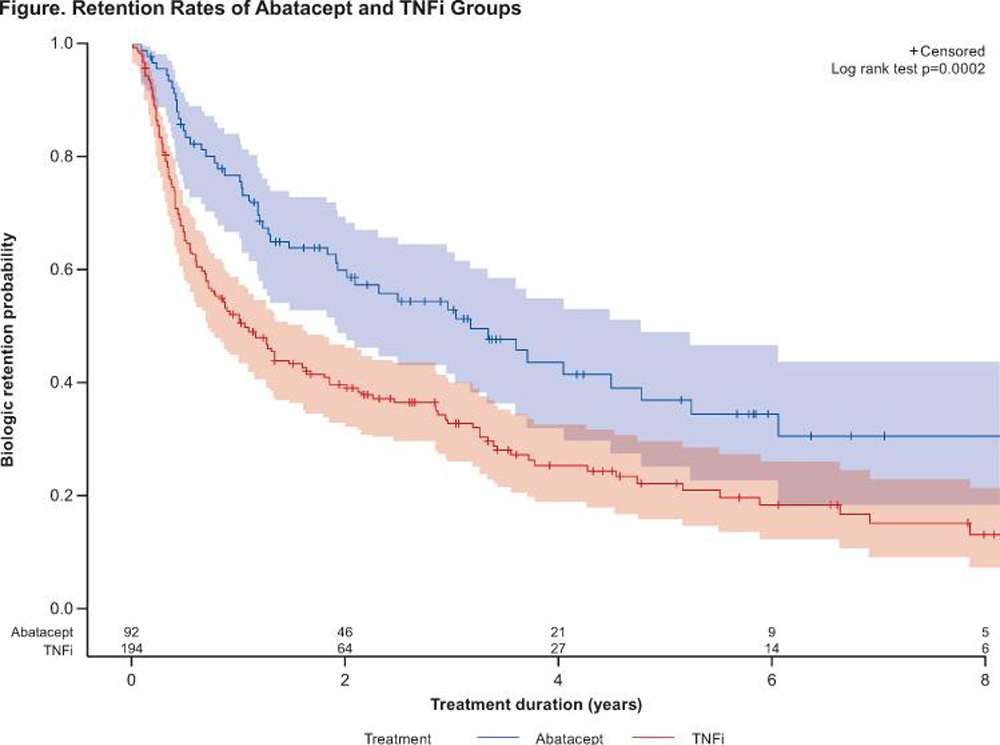
Conclusions: Abatacept has better sustainability over a second line TNFi in RA patients having failed one prior bDMARD.
Disclosure of Interest: D. Choquette Consultant for: BMS, Speakers bureau: BMS, L. Bessette Grant/research support from: Amgen, BMS, Janssen, Roche, UCB, AbbVie, Pfizer, Merck, Celgene, Sanofi, Lilly, Novartis, Consultant for: Amgen, BMS, Janssen, Roche, UCB, AbbVie, Pfizer, Celgene, Lilly, Novartis, E. Alemao Shareholder of: BMS, Employee of: BMS, B. Haraoui Grant/research support from: BMS, Janssen, Roche, Consultant for: Abbvie, Amgen, BMS, Celgene, Janssen, Merck, Pfizer, Roche, Sandoz, UCB, Speakers bureau: Pfizer, UCB, F. Massicotte: None declared, M. Mtibaa Shareholder of: BMS, Employee of: BMS, E. Muratti Employee of: BMS, J.-P. Pelletier: None declared, R. Postema Shareholder of: BMS, Employee of: BMS, J.-P. Raynauld Speakers bureau: AbbVie, Amgen, BMS, Janssen, Pfizer, Roche, Sanofi, Novartis, UCB, M.-A. Rémillard: None declared, D. Sauvageau: None declared, A. Turcotte Consultant for: Amgen, Abbvie, BMS, Celegene, Janssen, Roche, Pfizer, Lilly, Novartis, Merck, Sanofi, UCB, Speakers bureau: Amgen, Abbvie, BMS, Celegene, Janssen, Roche, Pfizer, Lilly, Novartis, Merck, Έ. Villeneuve Speakers bureau: Abbvie, Roche, BMS Consultant - Celgene, Cimzia, Pfizer, L. Coupal: None declared
DOI: 10.1136/annrheumdis-2017-eular.2379