fetching data ... 
Background: Sustainability of treatment is important to consider when selecting a therapy for chronic conditions such as RA. Sustainability is a useful clinical marker for both long-term efficacy and safety. A recently published randomized controlled trial has demonstrated similar efficacy and safety profiles between abatacept (ABA) and adalimumab over 2 years.1,2
Objectives: To assess the long-term sustainability of ABA and anti-TNFs following treatment failure with a conventional synthetic DMARD (csDMARD) in comparable cohorts of patients (pts) with RA.
Methods: Data from pts with RA seen at two tertiary centres and prescribed either ABA or a TNF inhibitor (adalimumab, certolizumab, etanercept, golimumab or infliximab) as their first biologic (b)DMARD after 1 January 2006 were extracted from the RHUMADATA® registry. The choice of therapy was a joint decision between the pt and the treating physician. Pts were followed until either they discontinued treatment, were lost to follow-up or the cut-off date of 9 January 2017. Pt baseline characteristics were compared using descriptive statistics and the cumulative incidence of biologic agent discontinuation using Kaplan-Meier methods. Overall differences in the discontinuation rates of biologic agents were tested using the log-rank test.
Results: Overall, 641 pts met study criteria; 82 pts received ABA and 559 TNF inhibitors (adalimumab=136, certolizumab=52, etanercept=226, golimumab=88 and infliximab=57) as first-line treatment following inadequate response to csDMARDs. No clinically significant differences in baseline characteristics were noted between treatment groups. Most pts were diagnosed after January 2000 (72.5%) and were women (77.5%). Average age at diagnosis was 47.1 (SD=13.4) years, with a mean disease duration of 7.2 (7.8) years, and a mean CDAI of 43.1 (32.5) at baseline. No significant differences in retention rates were observed in the ABA and anti-TNF groups (Table, Figure). On average, pts treated with anti-TNFs and ABA maintained their treatment for 1.59 (1.91) and 1.90 (2.08) years, respectively. Lack of efficacy (47.6%) and adverse effects (22.0%) were the most commonly cited reasons for treatment discontinuation.
Table 1. Retention of the first bDMARD *% (% standard error) survival.
TNFi Abatacept Biologic retention probability at*: 12 Months 71.66% (1.92%) 70.71% (5.15%) 24 Months 59.85% (2.11%) 62.16% (5.60%) 60 Months 44.28% (2.26%) 48.37% (6.75%) 96 Months 35.29% (2.46%) 41.17% (7.43%) bDMARD retention time (years) Mean (SE) 4.83 (0.18) 4.71 (0.45) Lower quartile, (95% CI) 0.86 (0.72–1.00) 0.86 (0.50–1.24) Median, (95% CI) 3.83 (2.87–4.67) 4.53 (2.34-++)
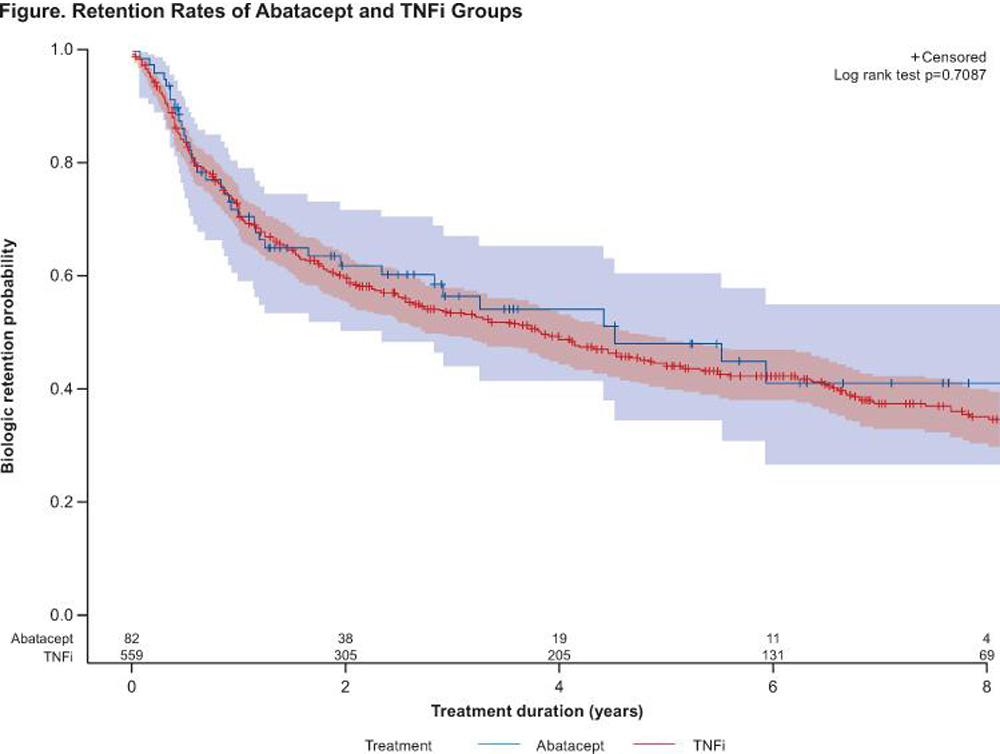
Conclusions: Abatacept and TNF inhibitors demonstrate similar sustainability at 8-year, supporting studies1,2 that demonstrate that abatacept used after csDMARDs inadequate response is as safe and effective as a TNF targeting agents in the long term.
References:
Schiff M, et al. Ann Rheum Dis 2014;73:86–94. Schiff M, et al. Ann Rheum Dis 2008;67:1096–1103.
Disclosure of Interest: D. Choquette Consultant for: BMS, Speakers bureau: BMS, L. Bessette Grant/research support from: Amgen, BMS, Janssen, Roche, UCB, AbbVie, Pfizer, Merck, Celgene, Sanofi, Lilly, Novartis, Consultant for: BMS, Janssen, Roche, UCB, AbbVie, Pfizer, Celgene, Lilly, Novartis, E. Alemao Shareholder of: BMS, Employee of: BMS, B. Haraoui Grant/research support from: BMS, Janssen, Roche, Consultant for: Abbvie, Amgen, BMS, Celgene, Janssen, Merck, Pfizer, Roche, Sandoz, UCB, Speakers bureau: Pfizer, UCB, F. Massicotte: None declared, M. Mtibaa Shareholder of: BMS, Employee of: BMS, E. Muratti Employee of: BMS, J.-P. Pelletier: None declared, R. Postema Shareholder of: BMS, Employee of: BMS, J.-P. Raynauld Speakers bureau: AbbVie, Amgen, BMS, Janssen, Pfizer, Roche, Sanofi, Novartis, UCB, M.-A. Rémillard: None declared, D. Sauvageau: None declared, A. Turcotte Consultant for: Amgen, Abbvie, BMS, Celegene, Janssen, Roche, Pfizer, Lilly, Novartis, Merck, Sanofi, UCB, Speakers bureau: Amgen, Abbvie, BMS, Celegene, Janssen, Roche, Pfizer, Lilly, Novartis, Merck, Έ. Villeneuve Consultant for: Celgene, Cimzia, Pfizer, Speakers bureau: Abbvie, Roche, BMS, L. Coupal: None declared
DOI: 10.1136/annrheumdis-2017-eular.2326