fetching data ... 
Background: Biosimilars and their reference agents have been shown to be equivalent in clinical trials. In the United Kingdom, etanercept biosimilars (ETA-B) are, since 2016, a first-line treatment option for the management of severe rheumatoid arthritis (RA) defined as no response to 2 or more csDMARDs. However, real world data, including how it compares to the etanercept originator (ETA-O) are lacking.
Objectives: This study aims to compare the short-term effectiveness of etanercept originator with its biosimilar in patients with RA when used as a first biologic following csDMARDs.
Methods: This study included patients with RA registered with the British Society for Rheumatology Biologics Registers for RA (BSRBR-RA) at the point of starting either ETA-O or an ETA-B since 2011 as their first biologic. Baseline information is collected at drug start and includes demographic and clinical data. Follow-up (FU) data are captured every 6 months and include details on therapy changes, current disease activity, and development of any adverse events. The primary outcome of this study is effectiveness as calculated by change in the 28 joint count disease activity score (DAS28). Only patients with a complete DAS28 at baseline and their 1st FU were included in the final analysis of this study. Hazard ratios (HR) comparing drug survival and risk of first serious adverse event (SAE) between ETA-O and ETA-B patients were calculated using Cox regression.
Results: Between January 2010 and 11 December 2017, 1217 and 412 patients starting ETA-O or ETA-B respectively were recruited and had ≥1 FU available. Complete DAS28 data at baseline and 1st FU were available for 740 ETA-O patients and 177 ETA-B patients. Patient characteristics were similar between the 2 cohorts (Table). After adjusting for baseline differences, no difference between groups was seen in DAS28 (p=0.1) or remission status (p=0.1) at 1st FU.
Nine (5%) and 48 (6%) of ETA-B and ETA-O patients had stopped their respective treatments by the 1st FU. The adjusted hazard ratio for stopping ETA-O versus ETA-B over this time period was similar (HR=0.8 (0.4-1.6); p=0.5). Risk of SAEs over the first 6 months was also similar between groups (HR (ETA-B versus ETA-O) =0.6 (0.3-1.1); p=0.1), with 10 (6%) and 73 (10%) SAEs reported in ETA-B and ETA-O patients respectively until 1st FU.
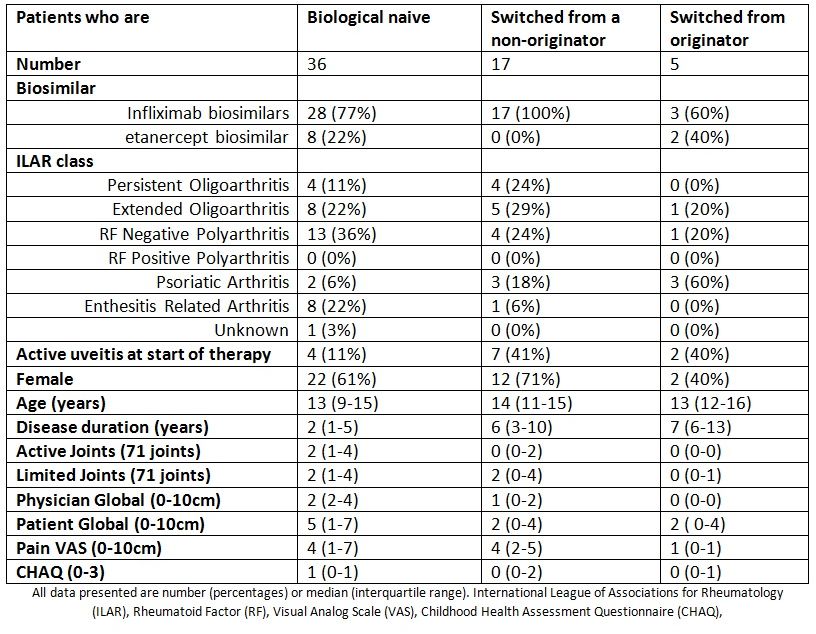
Abstract AB0429 – Table 1
Conclusions: In the UK, etanercept biosimilars are now frequently used as first-line biologics in RA patients. These short-term follow-up data demonstrate in routine clinical care that ETA-B appears to be equivalent to ETA-O in terms of short term effectiveness, drug survival and safety.
Disclosure of Interest: None declared
DOI: 10.1136/annrheumdis-2018-eular.4508